
1 2 gbs 2 3 Intracranial Hypotension Etiology reduced CSF pressure is precipitated by Surgery CSF over shunting or trauma including trivial fall Vigorous exercise or violent coughing ID: 933870
Download Presentation The PPT/PDF document "1 Hypothalamic hamartoma" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
1
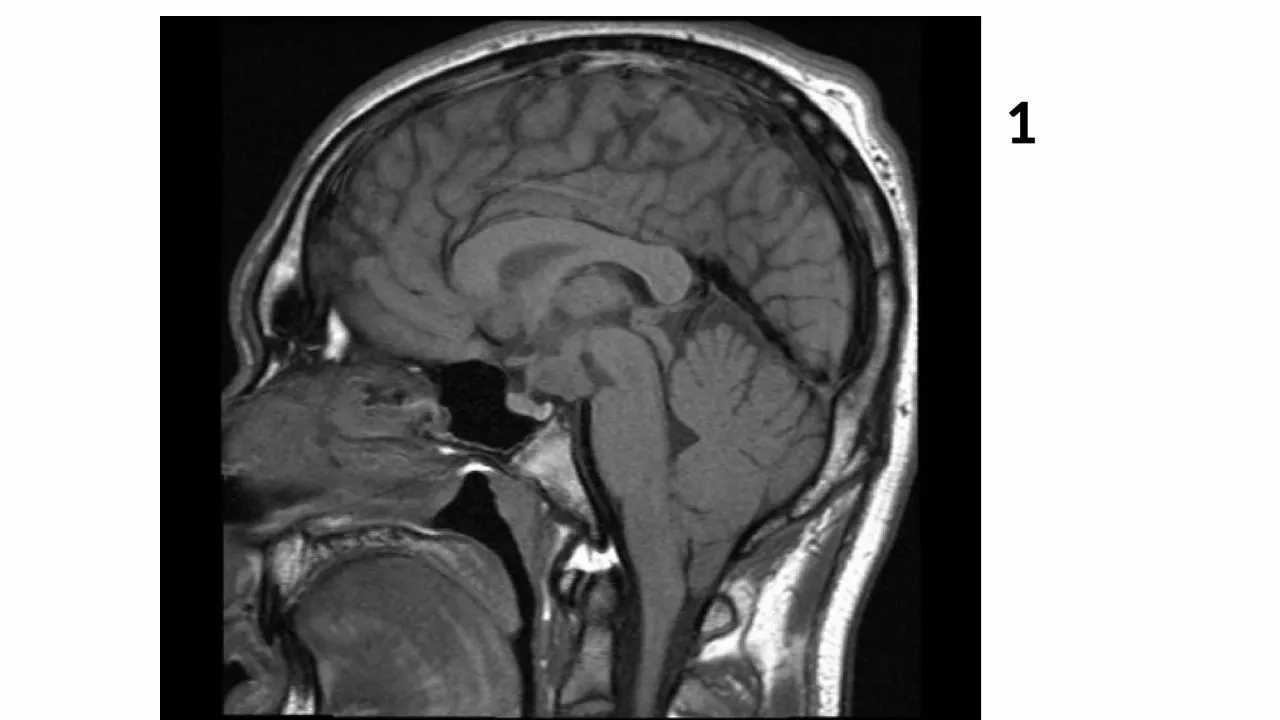
Slide2Hypothalamic
hamartoma
1
Slide32
Slide4gbs
2
Slide53
Slide6Intracranial Hypotension
Etiology: reduced CSF pressure is precipitated by
Surgery ( CSF over shunting) or trauma ( including trivial fall).
Vigorous exercise or violent coughing.
Diagnostic lumbar puncture.
Spontaneous dural tear, ruptured arachnoid diverticulum.
Severe dehydration.
Disc herniation or osteophytes (rare).
Classic Imaging features:
Downward displacement of brain through
incisura
( slumping midbrain).
Diffuse
dural
thickening/ enhancement.
Veins,
dural
sinuses distended.
Subdural
hygromas
/ hematomas.
3
Slide7Name
artefact
4
Slide8Phase wrap/aliasing
4
Slide95
Slide10Epidermoid
Epidermoid cysts comprise 0.2%–1.8% of primary intracranial
The most common location for epidermoid cysts is the cerebellopontine angle cistern (40%–50%), Epidermoid cysts also occur in the fourth ventricle (17%) and the sellar and/or parasellar regions (10%–15%).
CSF-like mass that insinuates within cisterns, encasing adjacent nerves and vessels.
On CT scans, most epidermoid cysts are well-defined hypoattenuated masses that resemble CSF and do not enhance. Calcification is present in 10%–25% of cases.
Isointense or slightly hyperintense to CSF on both T1- and T2-weighted MR images ,do not suppress completely on FLAIR images and restrict on diffusion-weighted images. Do not enhance, although some minimal rim enhancement occurs in approximately 25% of cases.
Rare “white epidermoids” have high protein content and may appear hyperattenuated on CT scans
5
Slide11A.CYST
EPIDERMOID
The major differential consideration for the epidermoid cyst is an arachnoid cyst. Arachnoid cysts are isointense to CSF at all sequences, including FLAIR. They displace rather than invade structures such as the epidermoid. Finally, arachnoid cysts do not restrict on diffusion-weighted images
5
Slide126
Slide13A
sbestosis
6
Slide147
Slide15Orbital blowout fractures
7
Slide168
Slide178
Slide18METASTATIC THYMIC CARCINOID
8
Slide19METASTATIC THYMIC CARCINOID
most common histologic type for a neuroendocrine tumour of the thymus.
ranges in differentiation and
behavior
from typical carcinoid to atypical carcinoid to small cell carcinoma.
50% of are functionally active -patients have Cushing syndrome as a result of
adrenocorticotropic
hormone secretion by the tumour -
ADRENAL HYPERPLASIA
carcinoid syndrome is uncommonLarge masses -propensity for local invasion. Focal areas of necrosis and punctate calcification may be present
8
Slide209
Slide21MYOSITIS OSSIFICANS
9
Slide2250 yr old female c/o progressive jaundice since 2 months
10
Slide23CHOLANGIOCARCINOMA
Cholangiocarcinoma is an adenocarcinoma that arises from the bile duct epithelium. It is the second most prevalent liver cancer after hepatocellular carcinoma
These three types of cholangiocarcinoma—extrahepatic, peripheral intrahepatic, and hilar intrahepatic
CT, -irregular mass with markedly low attenuation, minimal peripheral enhancement, and focal dilatation of intrahepatic ducts around the tumor. Thin, incomplete rim enhancement during both the arterial and portal venous phases.
The central part of the tumor does not enhance during these phases, whereas there may be prolonged enhancement at delayed-phase CT.
ancillary findings in peripheral cholangiocarcinoma include capsular retraction and dilatation ,Atrophy and thickening of the peripheral intrahepatic ducts
10
Slide2411
Slide25RETINOBLASTOMA
11
Slide265yr old with failure to thrive,
neurodevelopmental
delay,
pigmentary
retinopathy,
neurosensory
hearing loss, dental caries.
12
Slide27Cockyane
syndrome
rare autosomal recessive
dysmyelinating
disease.
Cinical
features include failure to thrive, developmental delay,
cutaneous
photosensitivity, pigmentary retinopathy, neurosensory hearing loss, dental caries, and
cachectic dwarfism. The diagnosis is considered very likely if the first 2 clinical criteria and at least 3 of the other criteria mentioned above are present.major brain atrophycalcifications in the basal ganglia (one of the causes of basal ganglial
calcifications in a child). Calcification may also occur in cerebellar and cerebral cortical region
lack of
myelination
of the white matter
12
Slide28MRI
There is atrophy which predominantly involves the
supratentorial
white matter, the cerebellum, the corpus callosum, and the brain
stem
.T2:
calcfication may be seen as low signal in putaminal, dentate nuclear and corticial regions The combination of
demyelination
and basal ganglia calcification may therefore be helpful in the imaging of this entity.
12
Slide2913
Slide3013
Slide3113
Slide3214
Slide33Mycotic aneurysm of aorta
Infected aneurysm (or mycotic aneurysm) is defined as an infectious break in the wall of an artery with formation of a blind, saccular out-pouching that is contiguous with the arterial lumen
Infected aneurysms are uncommon but can affect any artery The aorta, peripheral arteries, cerebral arteries, and visceral arteries are involved in descending order of frequency
Staphylococcus
and
Streptococcus
species are the most common causes of infected aneurysms
Infected aneurysms can develop from
(a)
hematogenous spread (b) infection of a preexisting intimal defect (c) contiguous involvement or (d)
direct infectious inoculation of the vessel
Early changes of aortitis preceding aneurysm formation include an irregular arterial wall, periaortic edema, a periaortic soft-tissue mass, and periaortic gas
14
Slide3415
Slide35MUCOPOLYSACHROIDOSIS
Macrocephaly
Delayed myelination
Dilated VR spaces
Hydrocephalous
White matter hyperintensities
J shaped sella
15
Slide3616
Slide37Congenital cystic
adenomatoid malformation
16
Slide3817
Slide39SINUS PERICRANII
Fluctuant scalp swelling
Communicating with underlying venous sinus through defect in skull
associated anomalies of deep venous system may be present
17
Slide4018
Slide41DIAGNOSIS
BASAL CELL NEVUS SYNDROME – GORLIN SYNDROME
Hereditary condition characterized by multiple basal cell carcinomas ,
Odontogenic keratocysts ,palmoplantar pits ,dural calcification ,medulloblastoma
18
Slide42RADIOLOGIC FEATURES
Odontogenic keratocysts in 80-90%,more common in mandible Calcification of falx in 100% ,calcified tentorium,dura and basal ganglia
Ventriculomegaly
Desmoplastic medulloblastoma
18
Slide4319
Slide44SARCOIDOSIS
The most common manifestation is bilateral hilar and mediastinal nodal enlargement, which is seen at some stage during the illness in over three quarters of patients . Classically the distribution is of bilateral hilar and right paratracheal nodal enlargement, which is known as the 1-2-3 SIGN or Garland triad
stage 0
: normal chest radiograph
5 - 10% of patients at presentation
stage I
: hilar or mediastinal nodal enlargement only
45 - 65% of patients at presentation
60% go onto complete resolution
stage II : nodal enlargement and parenchymal disease 25 - 30% of patients at presentation
stage III
: parenchymal disease only
15% of patients at presentation
stage IV
: end-stage lung (pulmonary fibrosis)
19
Slide45Parenchymal features are varied depending on the individual patient and the stage of disease
reticulonodular opacities most common : 75 - 90% of stage II and III cases .middle and upper zone distribution
bilateral and symmetric
nodularity may be prominent
airspace-like opacities (alveolar sarcoidosis )usually ill-defined and peripheral ,may appear mass-like actually represent interstitial rather than intra-alveolar process
coalescence of multiple ill-defined nodules
end-stage fibrosis occurs in approximately 20% of patients ,permanent coarse linear opacities ,typically radiating laterally from the hilum into the adjacent upper and middle zones ,upward and outward elevation of hila ,distortion of normal distribution of vessels and fissures
19
Slide4620
Slide47Organoaxial
volvulus
20
Slide4822 y old male presented with neck mass
Slide49Plunging
ranula