
Lecture 1 Mays Ibrahim Arab board of pathology CABP University of Al Mustansiriyah college of medicine Learning objectives You should Know what infectious diseases are and identify infectious agents ID: 930782
Download Presentation The PPT/PDF document "Infectious diseases pathology" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
Infectious diseases pathology Lecture 1
Mays Ibrahim, Arab board of pathology, CABPUniversity of Al-Mustansiriyah, college of medicine
Slide2Learning objectives
You should:Know what infectious diseases are and identify infectious agents.Understand
host barriers to infection and causes of failure of these barriers
.
Able to explain
types of inflammatory responses
to infection.
Slide3Infectious diseases are disorders in which tissue damage or dysfunction is produced by microorganisms.
Despite the availability and use of effective vaccines and antibiotics, infectious diseases remain an important health problem worldwide.The cooperation between humans and microorganisms is the rule; and disease is the exception.
The relationships between human and microorganisms are:
Symbiotic:
benefit of both partner
Commensal
: the microorganism shares the host’s food without causing harm
Slide4Infectious agents:
Prions: which are modified host proteins lacking genetic molecules.Viruses
: obligate intracellular organism which only replicate intracellularly (requiring host cell metabolism for replication.
Bacteria
: prokaryotes (lacking nucleic acid and endoplasmic reticulum) but have cell walls.
Fungi
Protozoa
: motile, single-celled eukaryotes.
Helminthes:
multicellular parasites with complicated life cycles often involving several hosts.
Ectoparasites:
bedbugs, fleas
Slide5Host barrier to infection
Slide6Host barrier to infection Skin
: normal defense in skin include epidermal barrier:Dense keratinized outer skin layer
Low PH of skin (5.5)
Presence of fatty acids within the layer of skin also inhibit microbial growth
Slide7Failure of local defense in skin occurs when there is:Mechanical defects (puncture, burn, ulcer)
Needle sticks (e.g. may transmit hepatitis B or C).Arthropods and animal bites.Direct penetration (e.g.
Schistosomiasis
).
Slide8Respiratory system: Normal defenses including
Hair of the nose and sneezingThe mucous layer secreted by the goblet cells in the nose and upper respiratory tract.
The
mucocilliary
clearance of the respiratory epithelium.
Mucosal immunoglobulin (IgA).
Alveolar macrophages and neutrophils recruited to the lungs by cytokines.
Slide9Note: large particles are trapped in the mucociliary
blanket that lines the nose and the upper respiratory tract, while particles smaller than 5 microns are carried into the alveoli, where they are phagocytized by alveolar macrophages or by neutrophils .Failure of local defense in respiratory system occurs when there is;
Mucociliary
clearance mechanism is disrupted (e.g., by smoking that cause metaplasia) or
hyperviscosus
mucus in cystic fibrosis
Host macrophage clearance is ineffective (e.g., in tuberculosis)
Attachment and local proliferation of microbes.
Slide10GIT:
Normal defenses against infected pathogens are:Epithelial barriers.Acidic gastric secretions.
Mucous secretions.
Bile and pancreatic enzymes.
Immunoglobulin A (IgA) antibodies, secreted by B cells located in the mucosa associated lymphoid tissues.
The normal protective gut flora.
Most gastrointestinal pathogens are transmitted by food or drink contaminated with
fecal material
Slide11Failure of local defense in GIT system occurs when there is;Attachment and local proliferation and invasion of microbes.
Acid-resistant cysts and eggs.Resistant microbial external coats.
Broad spectrum antibiotic use that affect the normal flora.
Slide12Urogenital tract:
Normal defenses against infected pathogens areFrequent bladder flushing with urine.Normal vaginal flora, catabolism of glycogen by normal commensal lactobacilli lowers the pH and reduces fungal growth.
Intact epithelial barrier.
Slide13Failure of local defense in urogenital system occurs when there is:
Bladder atonia, flow obstruction, or reflux.Antibiotics kill the lactobacilli and render the vagina susceptible to candidal infection.
Microbial attachment and local proliferation.
Direct infection/local invasion.
Local trauma (e.g. sexually transmitted diseases).
Slide14The transmission can beFrom person-to-person: via respiratory e.g
, T.B, fecal-oral e.g. HAV, sexual e.g. AIDS, or transplacental routes e.g. congenital Syphilis or through sharing neeedles. Animal-to-human trans- mission can occur through direct contact or ingestion (zoonotic infections).Insect or arthropod vectors may passively spread infection e.g., leishmaniasis
Slide15Immune evasion by microbes:After bypassing host tissue barriers, infectious microorganisms need to evade host immunity
Strategies include:Remaining inaccessible to host defense either in areas not reachable by antibodies or mononuclear cells (e.g GIT lumen or epidermis).
Antigenic variation
Inactivating antibodies or complement.
Resisting phagocytosis
, e.g. by producing a
capsule
Suppressing the host adaptive immune response, e.g. by interfering with cytokines or inhibiting MHC expression and antigen presentation.
Establishing
latency
, during which viruses survive in a silent state in infected cells.
Slide16How can the microorganism cause a disease?
Infectious disease results from the interaction of microbial virulence characteristics and host immune responses.
Infectious agents cause damage by:
• Entering cells and
directly causing cell death
.
• Releasing
toxins
that kill cells (microbial products including endotoxin, exotoxins or
superantigens
).
• Releasing
enzymes
that degrade tissue components
•
Damaging blood vessels
, causing ischemic necrosis
• Inducing
host inflammatory cell responses
that directly or indirectly injure tissues.
Slide17Spectrum of Inflammatory Responses to Infection:
Microbes produce 5 types of tissue reactions:Suppurative
(Purulent) Inflammation
Mononuclear & granulomatous inflammation
Cytopathic-cytoproliferative
response
Necrotizing inflammation
Chronic inflammation and scarring
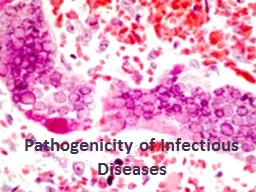
Slide18Slide19Suppurative (Purulent) Inflammation:
Is an acute tissue reaction to damage usually caused by pyogenic bacteria.
Pyogenic bacteria : is bacteria cause pus formation.
These elicit increased vascular permeability and
neutrophil
recruitment through
bacterial
chemoattractants
.
Massing of neutrophils and liquefactive necrosis of the tissue form
pus
.
E.g. consolidation of entire lung lobes in pneumonia; these may resolve without sequelae (pneumococcal pneumonia) or may scar (Klebsiella).
Slide20The alveolar architecture is still maintained, which is why even an extensive pneumonia often resolves with minimal residual destruction or damage to the pulmonary parenchyma
Slide21Mononuclear & granulomatous inflammationDiffuse, predominantly
mononuclear, interstitial infiltrates are a common feature of all chronic inflammatory processesBut when they develop acutely
, they often are response to
viruses.
For example:
plasma cells are abundant in syphilis
lymphocytes predominate in HBV infection.
Slide22Slide23Slide24Slide25Granulomatous inflammation
is a distinctive form of mononuclear inflammation characterized by accumulation of activated macrophages called “epithelioid” cells, which may fuse to form giant cells. In some cases there is a central area of caseous necrosis.
Cause:
Usually evoked by
infectious agents that resist eradication and are capable of stimulating strong T cell–mediated immunity
.
e.g., M. tuberculosis,
Histoplasma
capsulatum
,
schistosome
eggs.
Slide26DDX of chronic granulaomatous infections
T.BLeprosy (tuberculoid leprosy).
Schistosome eggs.
Histoplasma
capsulatum
Slide27Cytopathic-cytoproliferative response
These reactions are characteristic of viral mediated damage to the host cell & these include:Virus may replicate inside the cell
formation of viral aggregate which may be visible as inclusion bodies
e.g
Cytomegalovirus.
Virus may induce cells to fuse and form multinucleated cells (e.g., measles virus or herpes-viruses).
May cause focal cell damage
discohesion
of the epithelial cells
blister formation.
May cause proliferation of the epithelial cells,
e.g
warts that are caused by HPV.
May cause dysplastic changes and cancer formation.
Slide28nuclei contain large, eosinophilic inclusions surrounded by a clear halo, classic owel eye inclusion of CMV
Slide29Koilocytic changes in HPVproliferation of the epithelial cells
Slide30Slide31Necrotizing inflammationMicrobes that secrete
powerful toxins cause rapid and severe tissue necrosis often in the absence of inflammation. Examples:Clostridium perfringins that cause severe cell death just like (
coagulative
necrosis)
Slide32Slide33Chronic inflammation and scarring:
Many infections may end in chronic inflammation which can lead to either:
Complete healing, or:
Extensive scarring
e.g
chronic HBV infection may cause cirrhosis of the liver
Slide34Slide35Bacterial infection Staphylococcal S
treptococcal Tubeculosis Leprosy Syphilis
Slide36gram-positive cocci that cause acute diseases due to direct infection or due to the production of toxins. It is pyogenic infection. Commonly colonize the nares, and skin.Staph aureus infections can cause :Skin infections Boil or furuncle : the most common staph infection, a pocket of pus around the hair follicle.
Carbuncle: it is a more extensive lesion. As a cluster of boils that are connected to each other under skinCellulitis: infection of deep skin layers Impetigo: is a highly contagious painful rash that mainly affects children caused by staph.after a week of formation it bursts and develop honey colored crusts Or streptococcal infection) Toxin mediated disease
toxic shock syndrome, scalded skin syndrome, rapid onset food poisoning .
MRSA
(methicillin resistant S aureus) infection.
Bacteremia
Staphylococcal infection
Slide37Streptococcal infection:Are gram positive coccus grow in pairs or chain. They are classified according to the pattern of hemolysis on blood agarBeta hemolyticstrept:group A-s. pyogen(cause pharyngitis, scarlet fever,
erysepilas, impetigo, R.F.) and group B-S. agalactiae(colonize female genital tract).Alfa hemolytic: S. pneumonia(cause of community acquired pn.)Gamma hemolytic: normal oral flora but common cause of endocarditis.
Streptococcal infection
Slide38Cellulites:Acute painful suppurative spreading infection of deeper dermis and subcutaneous tissues. Often starts with a break in skin.Usually
from strept pyogens or staph aureusThe infection spread through the lymphatic leads to L.N swelling and tenderness of these L.N.Clinically:The affected area will be red, edematous, indurated with NO well defined margin.
Erysipelas:
infection involving upper dermis and superficial
lymphatics
, usually
from
strept
pyogens
NO suppuration unless deeply infected. Clinically:
The affected area has red, The rash has a sharp, well-demarcated border.
Types of streptococcal infection
Slide39Erysipelas
cellulitis
Slide40