
Khamaiseh FRCOG MRCP Consultant in OampG amp reproductive medicine Presence of pregnancy outside the uterine body Incidence 12 It used to be a significant cause of maternal mortality due to ID: 932317
Download Presentation The PPT/PDF document "Ectopic pregnancy Dr Khaldoun" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
Ectopic pregnancy
Dr
Khaldoun
Khamaiseh
FRCOG MRCP
Consultant in O&G & reproductive medicine
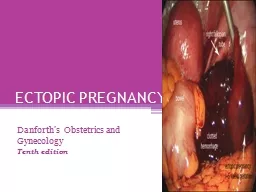
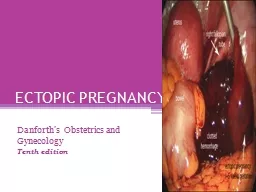
Slide2Presence of pregnancy outside the uterine bodyIncidence 1-2% . It used to be a significant cause of maternal mortality due to
haemorrhage
, now less due to early detection and management
Introduction
Slide3Slide4IUCD contraception failurePrevious tubal surgery including Tubal ligation
Previous ectopic pregnancy 15% after 1
ectopic and 25% after two ectopic
Progesterone
contraception failure
PID
Infertility
Risk factors
Slide5Tubal :95% (in the ampulla in 70% of cases)Ovarian
Cervical: 1 : 18000
Abdominal: attached to omentum
or rarely splenic or hepatic
Broad ligament
Sites of
ectopic
pregnancy
Slide6Quantitative B-HCG: If more than 6000 iu/l we should see intrauterine pregnancy by abdominal ultrasound, or more than 1500 IU/L we should see intrauterine G sac by
Transvagianl
USS, if not then it is an ectopic
Be careful of the pseudo sac
Less than 66% increase in BHCG after 48 hours is suggestive of ectopic or failed pregnancy
Gold
standrard is laparoscopy
Diagnosis
Slide7Slide8Slide9Slide10Slide11Usually 6-8 weeks Amenorrhoea
in 70%
Pain, unilateral pelvic pain. In 95% of casesPain could be dull ache due to distention of the tube or colicky spasmodic due to tubal abortion or generalized if ruptured with shoulder tip pain
Vaginal bleeding usually mild and dark (60%)
May be associated with dizziness and shock
presentation
Slide12AsymptomaticPelvic pain
Amenorrhoea
Vaginal bleedingCould present with shock if ruptured
Presentation
Slide13Local pelvic tenderness: unilateralCervical excitationUterus slightly enlarged
Mass in the pelvis felt by vaginal ex
Pallor and anemia if significant blood lossTachycaria
, hypotension and shock
Signs
Slide14Conservative expectant: wait for resorption of ectopic and declining B HCG level
Medical treatment: Methotrexate IM 50 mg/m square
Surgery: Mainly laparoscopy: Salpingectomy versus
salpingostomy
vs
salpingotomy
: depend if the other F. tube is present
Management
Slide15Slide16G sac size less than 3 cm with no cardiac activityBHCG less than
1500
IU/lNo intraperitoneal bleeding
Success 90%
Need to monitor CBC,LFT and (BHCG level declining), if decline less than 20% after 1 week can repeat dose
Should
avoid pregnancy for 6 months due to risk of teratogenicity
Criteria for medical management with methotrexate
Slide17Presence of both intrauterine and ectopic pregnancy in the same patient at the same timeVery rare 1:15000
But now more common with assisted conception 1 in 1000
Management : Remove the ectopic and the intrauterine pregnancy usually continues
Heterotopic pregnancy
Slide18Thank you