
Jakub Dębski Klinika Hematologii Nowotworów Krwi i Transplantacji Szpiku UM Wrocław Patient 1 Interview 59yearold patient with chronic lymphocytic leukemia diagnosed in 2009 in stadium ID: 930358
Download Presentation The PPT/PDF document "Emergencies in hematology" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





Slide1
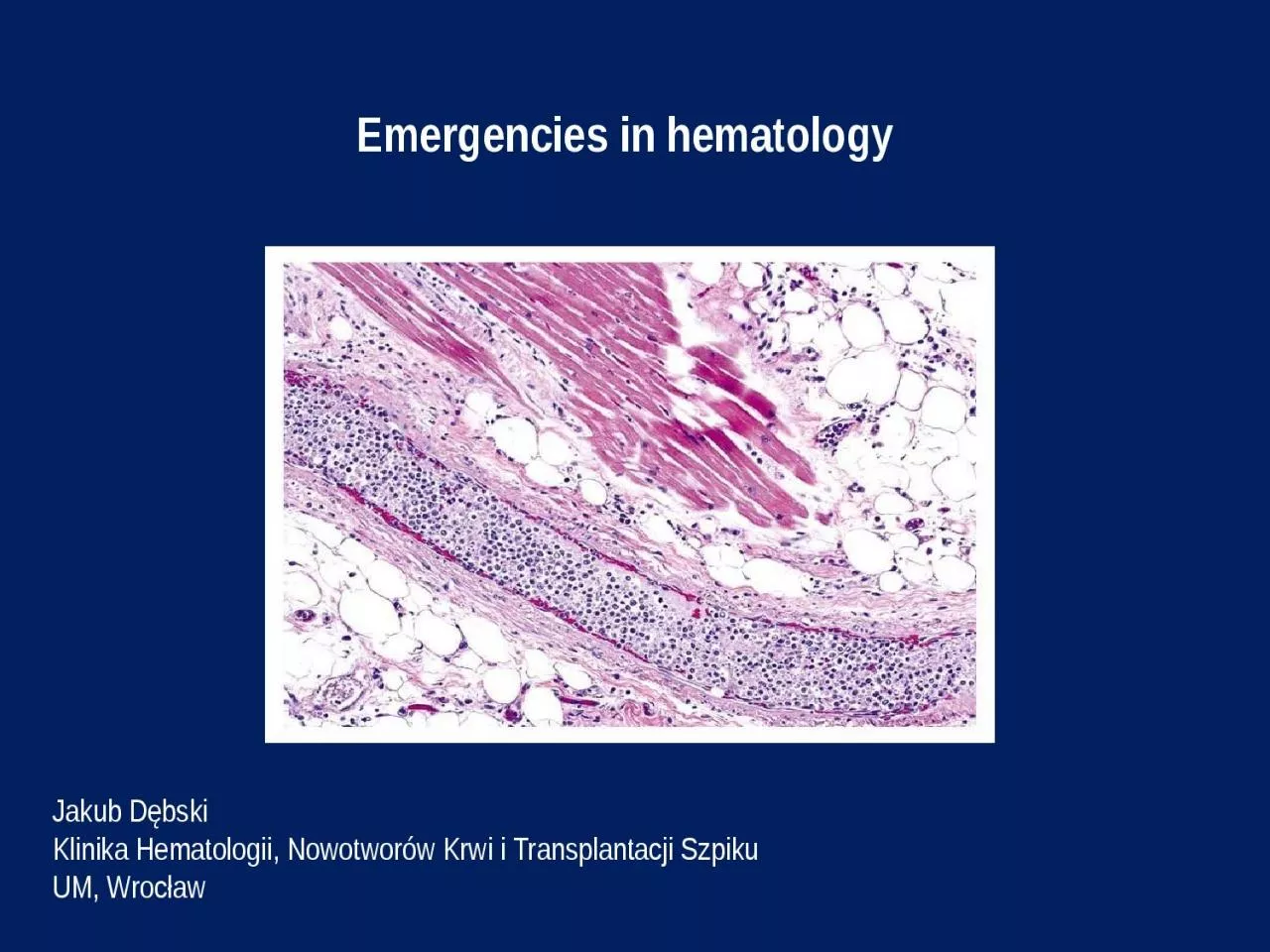
Emergencies in hematology
Jakub DębskiKlinika Hematologii, Nowotworów Krwi i Transplantacji SzpikuUM, Wrocław
Slide2Patient 1
Interview: 59-year-old patient with chronic lymphocytic leukemia diagnosed in 2009 in stadium - Rai II, Binet B was transferred from the Internal Medicine Department to the Department of Hematology for the treatment of pneumonia and significant progression of the disease. The patient who was previously untreated
hematologically, did not agree to the proposed chemotherapy during
several
visits
in
the
outpatient
clinics
- the last visit on
8.01.
2014. In March 2015, he was hospitalized
in
the
Surgery
Unit
due to
phlegmon
of
the
left
thigh
. Then
we
found
:
leukocytosis
800 G / l,
osteolytic
lesions of left
thigh
and pelvic
bones
, and in the performed on 17.03.2015 ultrasound examination of the abdominal cavity -
hepatosplenomegaly
with significantly enlarged lymph nodes, the largest with dimensions of 85 x 24 mm. The patient was advised to report urgently to the Hematology Clinic, but he did not. For about 3-4 days he
had
been
observ
ing
cough, weakness, fever up to 40
C. H
ospitalized
in
the
Internal
Medicine
Unit
between
29-30.04.
20
15
,
in
which
he
has been diagnosed with right-sided pneumonia with severe course and progression of untreated chronic lymphocytic leukemia.
Slide3Patient 1At the reception on 30.
04.2015:very severe condition, ECOG-3/4, drowsy, in a simple logical contact, conscious, aware, he
reported a worsening of vision.In
the
physical
examination
:
c
achectic
, right-sided rattling and crackling, left-sided crackles,
RHA
,
tachypnoe
22 /min,
abdomen
arched above the chest level, soft, tender, without peritoneal symptoms,
hepatosplenomegaly
, numerous lymph node packages palpable through the abdominal wall, lymph nodes
-
cervical,
axillary
, inguinal
–
enlarged
up to 2-3 cm in diameter, organized in packets,
n
umerous
scars and skin cavities of the left lower leg
due
to
the
phlegmon
(
cured
).
Slide4Patient 1Peripheral blood
morphology: WBC 982.77 10*3/uL [4-10] , IG% 0.3 % ,
NEUT% 1.6 % [40-75] , LYMPH% 89.4 % [25-45] ,
MONO% 9 % [2-12] ,
EO% 0 % [1-6] ,
BASO% 0 % ,
NRBC% 0 % ,
IG# 2.72 10*3/
uL
,
NEUT# 14.99 10*3/uL [1.6-7.5] , LYMPH# 878.61 10*3/uL [1-4] , MONO# 88.9 10*3/uL [0.08-1.2] , EO# 0.07 10*3/uL [0.04-0.6] , BASO# 0.2 10*3/uL [0-0.1] , NRBC# 0.41 10*3/uL , RBC 2.06 10*6/uL [4.5-5.9] , HGB 5.8 g/dL [14-18] , HCT 19.1 % [37-53] , MCV 92.7 fL [81-98] , MCH 28.2 pg [26-34] , MCHC 30.4 g/dL [31-37] , RDW-SD 63.2 fL [37-54] , RDW-CV % 18.9 % [11-16] , PLT 51 10*3/uL [130-400] , PDW 12.4 fL [9-17] , MPV 10 fL [9-13] , P-LCR 28.2 % [13-43] .
Slide5Patient 1In laboratory
tests:In peripheral blood morphology –
Leukocytes 982.77 G / l,Hemoglobin 5.8 g / dl,
Thrombocytes
51 G / l,?
Procalcitonin
36.02
ng
/ ml,
SaO2 82-84%,
Biochemistry – Increased level of glucose, CRP, LDH, urea, uric acid, ASPAT, ALP, total and direct bilirubin, magnesium, fibrinogen, D-dimers Decreased level of potassium, total protein, albuminWhat should be the further management of the patient?
Slide6Patient 1The course of treatment:The patient was
monitored, hydrated, and an urgent leukapheresis was performed followed by the first cycle of CVP (cyclophosphamide, vinblastine
) chemotherapy in fractionated doses along with intravenous corticosteroids. RBC concentrate
was
transfused
. In addition, broad-spectrum antibiotics and supportive care were used,
achieving
in the next days of stay an improvement in the general condition of the patient, along with moderate
cytoreduction
and a
significant decrease in inflammation parameters. Due to the rebound of leukocytosis on 8.05.2015, another leukapheresis procedure was performed and the second and third CVP chemotherapy courses were implemented on 8.05.15 and 28.05.15, followed by further cytoreduction and moderate reduction of the size of the lymph nodes, liver and spleen. Because of insufficient response achieved after the 3 cycles of CVP, the therapeutic protocol was changed to FC-R (fludarabine, cyclophosphamide, rituximab), the first cycle of which was introduced with good tolerance.
Slide7Patient 1Leukapheresis - a method
of selective mechanical purification of plasma from
morphotic elements -
leukocytes
(
granulocytes
,
monocytes
,
leukemic
blasts, CD34 + peripheral blood stem cells) using a separator.
Slide8Hyperleukocytosis
Definition: leukocytes > 100 G / lIt leads to complications
: LS - leukostasis
syndrome
DIC –
disseminated
intravascular
coagulation
TLS - tumor lysis syndromeThe risk of complications depends on the biology of leukemic cells.Epidemiology: - AML - acute myeloid leukemia (10-20%) - subtypes M4, M5, microgranular variant M3 - ALL - acute lymphoblastic leukemia (10-30%) - T-cell subtypes, males, infants, 10-20 years of age (rarely leukostasis syndrome) - BL - lymphoma / Burkitt's leukemia - mainly TLS- CLL - chronic
lymphocytic leukemia – symptomatic > 400 G / l (
rarely leucostatic
syndrome)
- CML -
chronic
myeloid
leukemia -
mainly
in
the
blast
crisis
phase
Slide9Leukostasis syndrome- symptomatic
hyperleukocytosis (clinical concept, not laboratory) - disturbances of blood flow and tissue perfusion as a result of accumulation of leukemic cells in the lumen of microcirculation vessels, often with activation of coagulation- most often affects the lungs (30%) and CNS (40%)Symptoms:
- dyspnoea, hypoxia
,
diffuse
vesicular
hemorrhage
,
acute respiratory failure (ARDS)- visual impairment, optic nerve edema, retinal hemorrhages - disturbances of consciousness, dizziness, tinnitus, drowsiness, headache, delirium, coma, focal neurological deficits, intracranial hemorrhage- myocardial ischemia / ACS- acute limb ischemia- renal vein thrombosis, exacerbation of preexisting renal failure- priapism- intestinal infarction
- fever (
due to cytokine
release or
associated
infection
)
-
progression
of respiratory
distress
sometimes
in
patients
after
the
start of
chemotherapy
, (
acute
lysis
pneumopathy
)
Slide10In laboratory tests:pseudohypoxemia
pseudohypoglycemiapseudohyperkalemiahypocalcaemia
hyperphosphatemiahyperuricaemia
lactic
acidosis
DIC
features
-
about
40% TLS features - about 10%Leukostasis syndrome
Slide11Leukostasis syndromeTreatment:
- urgent leukapheresis – 2 procedures with an interval of 12-24 hours
Diagnosis
Symptomatic
hyperleukocytosis
(G/l)
Asymptomatic
hyperleukocytosis
(G/l)AML 50 100ALL 150 300CML 150NoCLL 500NoAPLNoNoIndications for a leukapheresis:
Slide12Leukostasis syndromeTreatment:
- cytoreduction: hydroxycarbamide 50-100 mg / kg, usually 2-4 g / day
, reduction in
the
value
of
leukocytosis
by 50-80%
within
24-48 hours - chemotherapy inducing remission - implemented when leukocytes < 50 G / l- adequate hydration and prophylaxis of tumor lysis syndrome- management of the coexist. intravascular coagulation syndrome- RBC concentrate transfusions - cautiously, slowly during or after the leukapheresis procedure- Platelet concentrate transfusions - maintenance of PLT level > 20-30 G / l
- antibiotic
therapy
- glucocorticoids
Slide13Leukostasis syndromeContraindications to
leukapheresis:- acute promyelocytic leukemia
- cardiorespiratory insufficiency
-
severe
cardiac
diseases
-
severe coagulation disorders
Slide14Disseminated intravascular coagulation (DIC)
- 10-15% pts with generalized tumors
, 15% with leukemia -
generalized
activation
of
coagulation
with
fibrinolysis disorders + coagulopathy with consumption- in the clinical presentation: bleeding (60%) and thrombotic complications - 3 types of DIC accompanying tumors: procoagulant, hyperfibrinolytic, subclinical- diagnosis - serial analysis of platelet counts, PT and aPTT coagulation times, fibrin degradation markers: fibrin monomers, FDP, D-dimers, fibrinogen concentration
Slide15Disseminated intravascular coagulation (DIC)
Management: - treatment of the underlying
disease- transfusions
of
blood
products:
RBC
concentrate
-
when
there is a significant loss of bloodFFP 10-15 ml / kg - active bleeding and elongation > 1.5-fold aPTT or PTFFP 15 ml / kg every 12-24 h or cryoprecipitate 1 unit / 10 kg every 24 h - active bleeding and fibrinogen < 1.0 g / l Platelet concentrate 1-2 U / kg - PLT < 20 G / l or PLT < 50 G / l + hemorrhagic diathesis - heparin (controversial) - should be considered in cases with predominant thrombotic symptoms - fibrinolysis
inhibitors - tranexamic
acid 10-15 mg / kg in
DIC with enhanced
fibrinolysis
-
in
acute
promyelocytic
leukemia - DIC
with
hyperfibrinolysis
,
life-threatening
hemorrhagic
complications
in
about
5% (65%
intracranial
bleeding
/ 32%
pulmonary
bleeding
) –
required
application
of ATRA (
all-trans
retinoic
acid
)
or
ATO (
arsenic
trioxide
)
Slide16Tumor lysis syndrome (TLS)- life-threatening
metabolic syndrome resulting from
the rapid breakdown
of
cancer
cells
- high
proliferative
activity and high chemosensitivity of the tumor- spontaneous form - Burkitt's lymphoma, acute leukemia with high hyperleukocytosis - induced form - acute leukemia (ALL > 100 G / l, AML > 50 G / l), Burkitt's lymphoma, lymphoblastic lymphoma - renal failure increases the risk of TLS - metabolic disorders - hyperkalemia, hyperphosphatemia, hyperuricemia, hypocalcaemia, metabolic acidosis - symptoms - acute
renal failure,
arrhythmias /
sudden cardiac
death
,
hypotension
,
heart
failure
,
convulsions
,
neuromuscular
hyperactivity
Slide17Tumor lysis syndrome (TLS)Management:
1. prophylaxis - hydration 3 l / m2 / 24 h 0.9% NaCl +
allopurinol 600-900 mg / 24 h + eventually leukapheresis
2.
treatment
-
diuresis
forced
by a
loop diuretic > 3 l / 24 h, hourly 100 ml / h + allopurinol 500 mg / m2 / day - in the case of severe hyperuricaemia - rasburicase (recombinant xanthine oxidase) 0.2 mg / kg / day i.v. - hemodialysis in the development of acute renal failure - correction of electrolyte disturbances
Slide18Hypercalcemia- increased total
calcium concentrations > 2.6 mmol / l (10.5 mg / dl) or ionized
calcium > 1.25 mmol / l (5 mg / dl)
-
in
the
case
of protein
disorders (hypoproteinaemia, hypoalbuminaemia): calculation corrected calcium concentration (mg / dl) = [measured calcium concentration (mg / dl) - albumin concentration (g / dl)] + 4 - in hyperproteinemia - possible spurious hypercalcemia The most common causes are: - increased osteolysis in plasma cell myeloma- lymphomas and leukemia - paraneoplastic syndrome or severe osteolysis (PTH-independent
) or production of 1,25(OH)2D3
-
bone tissue
neoplasms
,
bone
metastases
-
primary
hyperparathyroidism
-
overdose
of
vitamin
D3
-
persistent
immobilization
-
thiazide
diuretics
,
theophylline
-
hyperthyroidism
-
adynamic
bone
disease
in
dialysis
patients
Slide19HypercalcemiaMild hypercalcemia < 3.0
mmol / l (12 mg / dl) - asymptomaticModerate and severe hypercalcemia
3.0 - 3.75 mmol / l (12-15 mg / dl) and rapidly
increasing
-
hypercalcemic
syndrome
:
1.
kidney problems - polyuria, hypercalciuria (nephrolithiasis, nephrocalcinosis)2. gastrointestinal symptoms - lack of appetite, nausea, vomiting, constipation, gastric / duodenal ulcer, pancreatitis, cholelithiasis3. cardiovascular symptoms - arterial hypertension, tachycardia, arrhythmia, hypersensitivity to digitalis glycosides4. neuromuscular symptoms - muscle weakness, weak tendon reflexes, transient facial
muscle paralysis
5. CNS symptoms
- headache, depression
,
orientation
disorders
,
drowsiness
,
coma
6.
dehydration
In a
very
severe
hypercalcemia
> 3.75
mmol
/ l (15 mg / dl) -
hypercalcemic
crisis
:
disturbances
of
consciousness
,
nausea
,
vomiting
,
abdominal
pain
,
arrhythmias
,
dehydration
,
death
.
ECG - prolongation of the PQ interval, QT shortening, wide T wave,sometimes the Osborn wave
Slide20HypercalcemiaManagement:- abundant
hydration - 3-5 liters / day (~ 3 l / m2 / day) 0.9%
NaCl- forced
diuresis
with
furosemide
20-40 mg iv,
diuresis: 150-200 ml / h - reducing the calcium release from bones - calcitonin 100 UI 2-4 times a day iv or bisphosphonates (eg. pamidronate 60-90 mg / 2 h iv or zoledronate 4 mg / 15 min iv) or denosumab- inhibition of calcium absorption from the gastrointestinal tract - glucocorticosteroids (eg. hydrocortisone 100 mg iv every 6 h)- in severe cases – hemodialysisIn
chronic tumor hypercalcemia
in addition
:- mitramycin
25
ug
/ kg for 4-6 h
i.v
.
or
-
gallium
nitrate
100-200 mg / m2 for 24
hours
for 4-5
days
Slide21Superior vena cava syndrome (SVCS)
- syndrome of symptoms caused by impeding blood flow from the superior vena cava to the right atrium of the heart- 2-4% of patients with lung cancer and 2-4% with lymphoma
The most frequent causes:- narrowing of the superior vena cava
1.
external pressure + tumor infiltration of the vein wall
-
lung cancer (60-80%), lymphoma (10-15%), metastasis of breast cancer,
mediastinal
germ cell tumors, thymomas 2. non-neoplastic causes - aortic aneurysm, chronic mediastinitis- superior vena cava thrombosis - a catheter or secondary mediastinal tumor- right atrial tumor (rare)
Slide22Superior vena cava syndrome (SVCS)
Symptoms:- swelling, erythema or bruising of the face
- conjunctival hyperemia
- swelling of the upper limbs
- symptoms associated with increased intracranial pressure: headache and dizziness, visual disturbances, convulsions
- permanent
distention
of the jugular veins and positive Pemberton
’s
sign - dyspnea- hoarseness- difficulty in swallowing- stridorThe chest CT scan is the test of choice to diagnose SVCS.Chest X-ray is normal in 5-15% of cases.
Slide23Superior vena cava syndrome (SVCS)
Symptomatic treatment:- dexamethasone 16-32 mg / d i.v
. for 7 days, then dose reduction- control of dyspnea
- morphine,
midazolam
, oxygen therapy
- loop diuretic
(eg.
furosemide
)
- low molecular weight heparin - prophylactic or curativeCausative treatment:- urgent irradiation of the mediastinum - in the majority of cancers, the treatment of choice - chemotherapy - for chemosensitive cancers: lymphomas, lung cancer, germ cell tumors - introduction of the stent into the superior vena cava (removal of symptoms in > 75% of patients within 48 -72 h after surgery)- in the case of thrombosis - also consider thrombolysis
Slide24Differentiation syndrome in acute
promyelocytic leukemia- life-threatening complication of the induction of acute myeloid leukemia M3 (promyelocytic)
after application of ATRA or ATO- occurs in
up
to
25% of patients within 7-12
days
of starting treatment
-
pathomechanism
is not known, probably cytokine-related- symptoms: fever, increasing dyspnea, peripheral edema, skin rash, lung infiltration, fluid in the pleural cavity and pericardium, hypotension, renal insufficiency- risk increased by leukocytosis > 50 G / l - treatment: dexamethasone 2 x 10 mg iv until the symptoms disappear, sometimes dialysis is necessary and respiratory therapy- in patients with severe organ-related complications - temporary withdrawal of ATRA or ATO- mortality is around 1%
Slide25Neutropenic fever n
eutropenia is the most common complication of anticancer treatment, it results from the myelotoxic action of chemo-radiotherapy or bone marrow infiltration by tumor cells- neutropenic fever - 10-50% of patients with solid tumors,
> 80% with hematological malignancies
Definition of
neutropenic
fever
(
febrile
neutropenia): 1. oral temperature ≥ 38.3 C in single measurement or ≥ 38 C persistent for 1 hour 2. neutrophil count < 500 / ul or predicted decrease to < 500 / ul in 48 hoursPatients with NF rarely have local infection or they are weakly expressed. Most often, bacterial infections (Gram +> Gram-), less often fungal and viral.Blood-borne infection - 13-60% of patients, mortality 12-42%. The most serious forms of infection are: pneumonia, neutropenic enteritis, septic shock.
Slide26Neutropenic feverManagement:
- broad-spectrum, wide-spectrum empiric antibiotic therapy, in patients at high risk of complications and death: carbapenem or piperacillin with tazobactam or
ceftazidime or cefepime iv
- addition of antifungal medication
(
eg
.
fluconazole
iv
) - microbiological tests - identification of the pathogen responsible for infection is successful in 20-30% of patients- use of granulocyte growth factors G-CSF or GM-CSF, if the patient did not receive them as a primary or secondary prophylaxisRegular assessment of the patient's condition, effectiveness of antibiotic therapy, development of complications every 24-48 hours is mandatory.In case of improvement or identification of an infectious agent - de-escalation of antibiotic therapy.
Slide27Prophylaxis in afebrile patients with neutropenia1) a
sanitary regime, hand and cough hygiene
, sometimes patient
isolation
2)
prophylactic
use
of
fluoroquinolone (ciprofloxacin, levofloxacin) - only in high-risk patients 3) prophylactic use of antifungal drugs (azoles, echinocandins) and antivirals (aciclovir) - only in patients undergoing allo-HCT and inducing remission chemotherapy in acute myeloid leukemia4) prophylactic use of cotrimoxazole in patients with risk factors
for Pneumocystis jiroveci
infection
- purine analogs
,
corticotherapy
> 1
month
5)
prophylaxis
with
G-CSF
(
filgrastim
,
lenograstim
)
or
GM-CSF
(
molgramostim
,
regramostim
,
sargramostim
):
-
primary
-
recommended
already
during
the
first
cycle
of
chemotherapy
,
when
the risk of developing febrile neutropenia > 20%, to consider also in the case of intensive
chemotherapy
-
secondary
-
recommended
in
patients
with
complications
associated
with
neutropenia
that
occurred
after
the
first
chemotherapy
cycle
, and
reducing
the
doses
of
cytotoxic
drugs
or
delaying
their
administration
may
affect
overall
survival
6)
avoidance
of
prolonged
environmental
contact
a high
concentration
of
fungal
mold
spores
(
constructions
, old and
neglected
buildings
)