
Peeranut Pholvicha MD Introduction Chronic hypertension Prehypertension Stage 1 hypertension Stage 2 hypertension Hypertensive emergency BP 180120 with endorgan damage Hypertensive urgency ID: 930992
Download Presentation The PPT/PDF document "Topic review : Systemic Hypertension" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






Slide1
Topic review : Systemic Hypertension
Peeranut
Pholvicha
, M.D.
Slide2Introduction
Chronic hypertension
Prehypertension
Stage 1 hypertension
Stage 2 hypertension
Hypertensive emergency
BP ≥ 180/120 with end-organ damage
Hypertensive urgency
BP ≥ 180/120 without end-organ damage
Slide3Classification
Slide4Classification
Slide5Classification
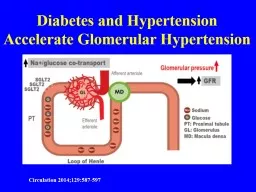
Slide6Pathophysiology
Slide7Cause of secondary hypertension
Slide8Cause of secondary hypertension
Slide9Slide10Slide11Slide12Slide13Slide14BP difference
BP measurement in both arms while resting
Check BP several times before start anti-HT
BP differences can result from many cause
Most important factor is increasing age
Mortality increasing in each 10 mmHg difference
Treat higher BP when difference is detected
Slide15Slide16Clinical features
Slide17Slide18Slide19Clinical features
Chest pain and severe HT
ACS vs uncommon aortic dissection
Rapid
diagnosis and treatment of acute aortic dissection are
critical
Abrupt, sudden onset chest pain (tearing or ripping) and radiating to
interscapular
region
25% have widening mediastinum in CXR
CT chest is the diagnosis of choice for dissection
Slide20Clinical features
Acute neurologic symptoms and severe hypertension
Elevated BP, headache and focal neurologic deficits > ischemic/hemorrhagic stroke
Diagnose with CT/MRI
Altered mental status, headache, N/V, seizures or visual disturbance > hypertensive encephalopathy (after excluding strokes)
Slide21Clinical features
Acute renal failure, peripheral edema and severe HT
Peripheral edema, oliguria, loss of appetite, N/V or confusion
Elevated Cr confirm diagnosis (urine sediment also abnormal)
Pre-
ecclampsia
> HT, peripheral edema and proteinuria and may develop hemolysis, elevated liver enzyme and low platelets (HELLP syndrome)
Slide22Clinical features
Sympathetic crisis and severe HT
Abrupt discontinuation of
Clonidine
Pheochromocytoma
> life-threatening HT > headache, alternate periods of HT and normal BP, tachycardia and flushed skin
Sympathomimetic drugs
> precipitated HT with tachycardia, diaphoresis, chest pain and mental status change (depend on agents)
Slide23Clinical features
Sympathetic crisis and severe HT
MAOi
> consume tyramine-containing food may develop a
hyperadrenergic
state
Autonomic dysfunction
> spinal cord or severe head injury or spina bifida injury may present as HT emergency
Slide24Clinical features
Asymptomatic patients with severe HT
No formal recommendations for evaluation
Basic metabolic panel, ECG, CXR and U/A
Evaluation
on the patient complaint, history, and review of
systems and perform
selected testing
Slide25Investigations
Slide26Slide27Treatment
Aortic dissection
Goal SBP 100-140 mmHg, HR ≤ 60
Inadequate BP and HR control outweighs risk of hypotension
Decrease shearing force and aortic wall stress
Opioids help decrease sympathetic tone
Slide28Treatment
Acute hypertensive pulmonary
edema
Nitrates reduce BP, decrease myocardial O
2
consumption and improve coronary blood flow
Diuretics improve symptoms but not affect mortality
Nicardipine
increases both stroke volume and coronary blood flow in systolic dysfunction
Pulmonary edema from ACS or AF with RVR > β-blocker
Slide29Treatment
Acute myocardial infarction
Nitrates in severe elevate BP and ischemic changes on ECG
β-blocker remains part of early care (IV only in severe HT)
Slide30Treatment
Acute sympathetic crisis
Decrease adrenergic stimulation with IV
benzodiazepines in cocaine or amphetamine use
(Nitroglycerine or
phentolamine
if not effective
)
CCB as third line
β-blocker can result in
α
-blockade > worsen coronary
vasocontriction
Slide31Treatment
Acute sympathetic crisis
IV
phentolamine
in
pheochromocytoma
with HT emergency
HT but not crisis in preoperative setting > oral
phenoxybenzamine
(long acting adrenergic
α
-blocker)
IV benzodiazepine in
MAOi
toxicity (
phentolamine
, NTG or
nitroprusside
it not respond)
Monitor closely after reach target BP
Slide32Treatment
Acute renal failure
Fenoldopam
> 1
st
line agent > improve
natriuresis
and
CrCl
Nicardipine
and
clevidipine
both suitable for acute HT induced renal failure
Slide33Treatment
Neurologic emergencies
Hypertensive encephalopathy is an indication for rapid BP reduction (once strokes are excluded)
IV
nicardipine
,
labetelol
,
fenoldopam
and
clevidipine
are all appropriate
NTG dilates cerebral arteries and alters blood flow > worsen auto-regulation failure
Slide34Treatment
Neurologic emergencies
Balanced BP control in strokes to avoid worsening ischemia or
rebleeding
Fibrinolytic
therapy is contraindicated in BP > 185/110 after anti-HT therapy
Monitor BP q 15 min for 2 hours from the start of r-TPA then q 15 min for 6 hours and then q 1 hour for 16 hours (Keep ≤ 180/105)
Slide35Treatment
Slide36Treatment
Slide37Treatment
Slide38Treatment
Slide39Treatment
Slide40Treatment
Slide41Pharmacologic agents
β-blockers
Labetelol
is recommend for nearly all HT emergencies (except for cocaine intoxication and systolic dysfunction with HF)
Metoprolol
indicated in ACS (benefit in terms of survival)
Esmolol
has short duration of action > advantage in those with severe asthma and COPD
Slide42Pharmacologic agents
Calcium channel blockers
Clevidipine
: ultra-short acting selective arteriolar vasodilator (half life < a minute)
Nicardipine
: safe and effective in neurologic HT emergencies, favorable effect on myocardial oxygen balance
Nifedipine
: not recommend in HT emergencies except in
peripartum
patients
Slide43Pharmacologic agents
Vasodilators
Nitroglycerin : potent
venodilator
, used as first line agent only in HF and ACS (favorable effects on coronary blood flow and cardiac work load) but can reduce preload and cardiac output
Sodium
nitroprusside
: best when other agents fail, possible cyanide toxicity in renal/hepatic insufficiency and combination therapy is the most
common current use
Slide44Pharmacologic agents
Slide45Pharmacologic agents
Slide46Pharmacologic agents
Slide47Pharmacologic agents
Slide48Pharmacologic agents
Slide49Slide50