
Aim To provide a guideline for the management of the post oesophagectomy patient Scope All adult critical care patients post oesophagectomy oesophogastrectomy M MacKinnon 30112016 ID: 934678
Download Presentation The PPT/PDF document "Oesophagectomy in Critical Care" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
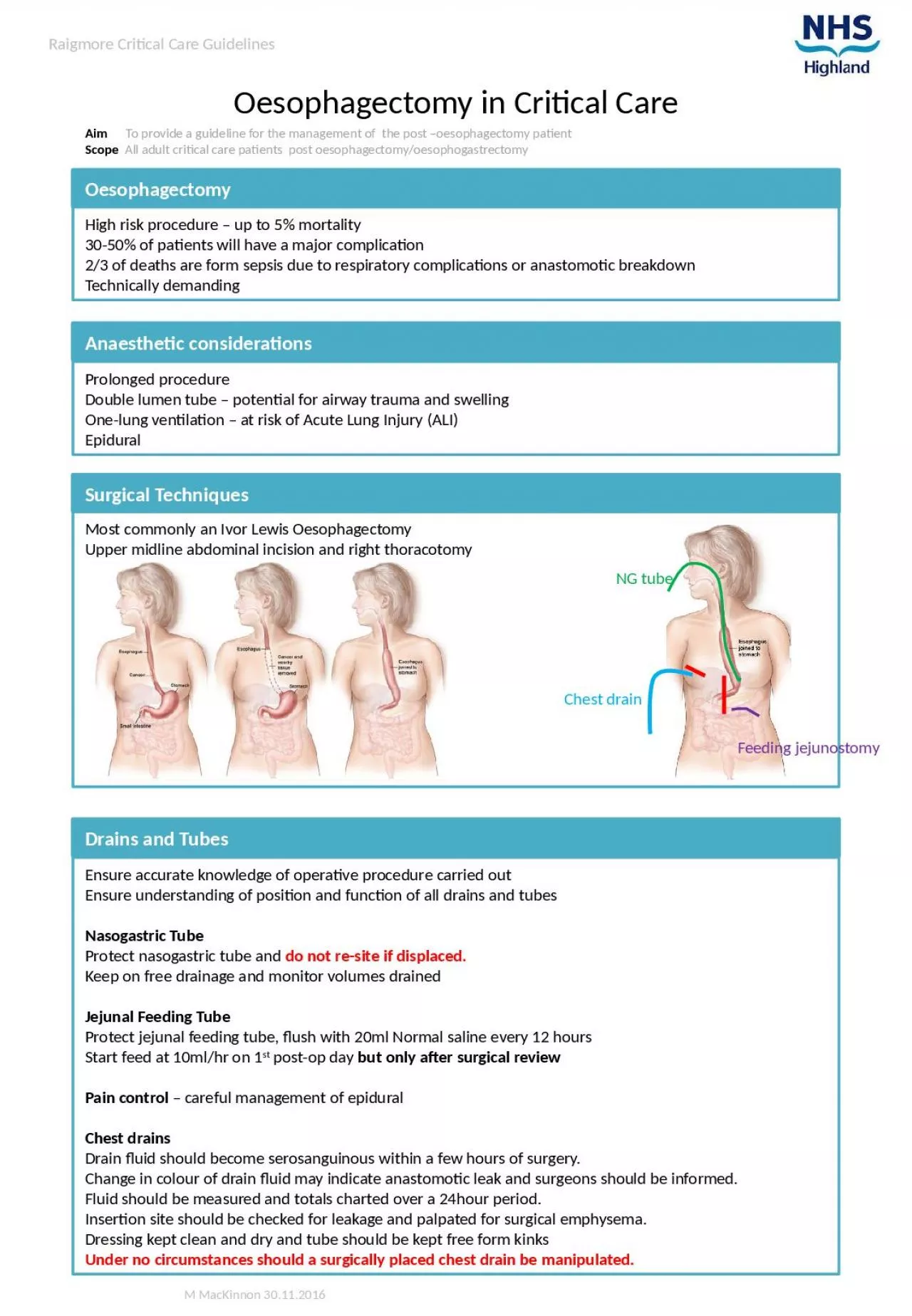
Oesophagectomy in Critical Care
Aim To provide a guideline for the management of the post –oesophagectomy patientScope All adult critical care patients post oesophagectomy/oesophogastrectomy
M MacKinnon 30.11.2016
Raigmore Critical Care Guidelines
Anaesthetic considerations
Prolonged procedure
Double lumen tube – potential for airway trauma and swellingOne-lung ventilation – at risk of Acute Lung Injury (ALI)Epidural
Oesophagectomy
Drains and Tubes
Surgical Techniques
Ensure accurate knowledge of operative procedure carried outEnsure understanding of position and function of all drains and tubesNasogastric TubeProtect nasogastric tube and do not re-site if displaced.Keep on free drainage and monitor volumes drainedJejunal Feeding TubeProtect jejunal feeding tube, flush with 20ml Normal saline every 12 hoursStart feed at 10ml/hr on 1st post-op day but only after surgical reviewPain control – careful management of epiduralChest drainsDrain fluid should become serosanguinous within a few hours of surgery.Change in colour of drain fluid may indicate anastomotic leak and surgeons should be informed.Fluid should be measured and totals charted over a 24hour period.Insertion site should be checked for leakage and palpated for surgical emphysema.Dressing kept clean and dry and tube should be kept free form kinksUnder no circumstances should a surgically placed chest drain be manipulated.
High risk procedure – up to 5% mortality30-50% of patients will have a major complication2/3 of deaths are form sepsis due to respiratory complications or anastomotic breakdownTechnically demanding
Most commonly an Ivor Lewis OesophagectomyUpper midline abdominal incision and right thoracotomy
NG tube
Chest drain
Feeding
jejunostomy
Slide2M MacKinnon 21.03.2017
Raigmore Critical Care GuidelinesRespiratoryAt risk of atelectasis and acute noncardiogeneic pulmonary oedemaClose monitoring of gas exchangeGeneral Measures
Early mobilisationHb >/= 75mg/lNormothermiaMAP target appropriate to pre-op valuesAnalgesia
Regular iv paracetamolEpidural as per chart
General Measures
Lungs at risk of ALI after OLV, handling, SIRS
Known that a positive balance on post-op day 1 is associated with significantly more pulmonary complications1Positive balance of >6000ml on Day 0 and accrued balance >5500ml by post-op day 4 are associated with morbidity.2Aim for UOP 0.5ml/Kg/hr
Fluid balance
J Thoracic Disease 2015;7(11):1986-1993Glatz
et al BMC Surgery (2017) 17:6Specific
Bleeding Oesophageal anastomotic leakFever, subcutaneous emphysema, unexplained tachycardia/tachypnoea, hypoxia, change in colour of chest drain fluid.Gastric necrosisFever, oliguria, acidosis, tachycardia, hypotensionRespiratory: Pneumonia, ARDS, AtelectasisTachypnoea, fever, hypoxaemia, new CXR infiltrates, confusionGeneralDVT/PE, Cardiac Arrhythmias, AMI, prolonged ileus, wound infection, gastrointestinal bleeding, diarrhoea, chylothorax.Complications