
Characteristics in seven sites from the CCASAnet Cohort IeDEA Region 2 Valeria Fink 1 Bryan Shepherd 2 Firas Wehbe 3 Claudia Cortés 4 Brenda Crabtree 5 Denis Padgett ID: 933841
Download Presentation The PPT/PDF document "Cancer in HIV Patients in Latin America ..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Cancer in HIV Patients in Latin America and the Caribbean: Characteristics in seven sites from the CCASAnet Cohort (IeDEA Region 2)
Valeria Fink1, Bryan Shepherd2, Firas Wehbe3, Claudia Cortés4, Brenda Crabtree5, Denis Padgett6, Maryam Shafaee7, Mauro Schechter8, Eduardo Gotuzzo9, Carina Cesar1, Alejandro Krolewiecki1, Melanie Bacon10, Catherine McGowan11, Pedro Cahn1, Daniel Masys121Fundación Huésped, Investigaciones Clínicas, Buenos Aires, Argentina2Vanderbilt University, Biostatistics, Nashville, United States3Vanderbilt University, Nashville, United States4Universidad de Chile- Fundación Arriarán, Santiago, Chile5Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubiran, Mexico, Mexico6Instituto Hondureño de Seguro Social y Hospital Escuela, Tegucigalpa, Honduras7GHESKIO/ Weill Medical College of Cornell University, Port au Prince, Haiti8Universidade Federal do Rio de Janeiro, Projeto Praça Onze, Rio de Janeiro, Brazil9Instituto de Medicina Tropical Alexander von Humboldt, Lima, Peru10HJF-NIAID/DAIDS, Epidemiology, Bethesda, United States11University of Vanderbilt, Infectious Diseases, Nashville, United States12University of Vanderbilt, Biomedical Informatics, Nashville, United StatesAcknowledgements: CCASAnet, IeDEA Region 2: Caribbean, Central and South AmericaSupport from NIH Cooperative Agreement 1-U01-AI069923 and 1-UL1-RR024975 from NCRR/NIH)
BACKGROUND
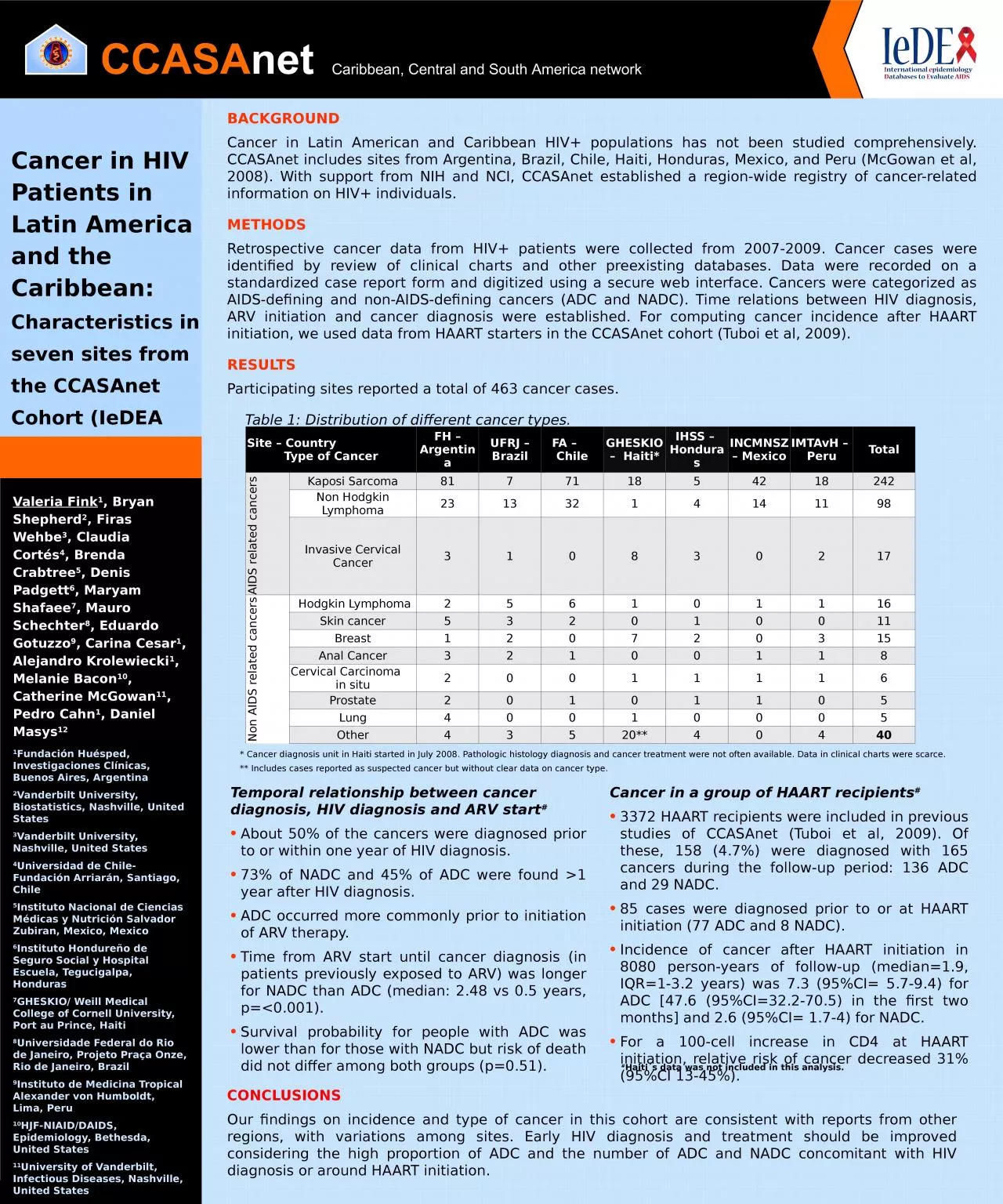
Cancer in Latin American and Caribbean HIV+ populations has not been studied comprehensively. CCASAnet includes sites from Argentina, Brazil, Chile, Haiti, Honduras, Mexico, and Peru (McGowan et al, 2008). With support from NIH and NCI, CCASAnet established a region-wide registry of cancer-related information on HIV+ individuals. METHODS Retrospective cancer data from HIV+ patients were collected from 2007-2009. Cancer cases were identified by review of clinical charts and other preexisting databases. Data were recorded on a standardized case report form and digitized using a secure web interface. Cancers were categorized as AIDS-defining and non-AIDS-defining cancers (ADC and NADC). Time relations between HIV diagnosis, ARV initiation and cancer diagnosis were established. For computing cancer incidence after HAART initiation, we used data from HAART starters in the CCASAnet cohort (Tuboi et al, 2009). RESULTS Participating sites reported a total of 463 cancer cases. Table 1: Distribution of different cancer types.
CONCLUSIONSOur findings on incidence and type of cancer in this cohort are consistent with reports from other regions, with variations among sites. Early HIV diagnosis and treatment should be improved considering the high proportion of ADC and the number of ADC and NADC concomitant with HIV diagnosis or around HAART initiation.
* Cancer diagnosis unit in Haiti started in July 2008. Pathologic histology diagnosis and cancer treatment were not often available. Data in clinical charts were scarce. ** Includes cases reported as suspected cancer but without clear data on cancer type.
Site – Country Type of CancerFH – ArgentinaUFRJ – BrazilFA – ChileGHESKIO – Haiti*IHSS – HondurasINCMNSZ – MexicoIMTAvH – PeruTotalAIDS related cancers Kaposi Sarcoma817711854218242Non Hodgkin Lymphoma23133214141198Invasive Cervical Cancer310830217Non AIDS related cancers Hodgkin Lymphoma256101116Skin cancer532010011Breast120720315Anal Cancer32100118Cervical Carcinoma in situ20011116Prostate20101105Lung40010005Other43520**40440
Temporal relationship between cancer diagnosis, HIV diagnosis and ARV start#About 50% of the cancers were diagnosed prior to or within one year of HIV diagnosis. 73% of NADC and 45% of ADC were found >1 year after HIV diagnosis. ADC occurred more commonly prior to initiation of ARV therapy. Time from ARV start until cancer diagnosis (in patients previously exposed to ARV) was longer for NADC than ADC (median: 2.48 vs 0.5 years, p=<0.001). Survival probability for people with ADC was lower than for those with NADC but risk of death did not differ among both groups (p=0.51).
Cancer in a group of HAART recipients#3372 HAART recipients were included in previous studies of CCASAnet (Tuboi et al, 2009). Of these, 158 (4.7%) were diagnosed with 165 cancers during the follow-up period: 136 ADC and 29 NADC. 85 cases were diagnosed prior to or at HAART initiation (77 ADC and 8 NADC). Incidence of cancer after HAART initiation in 8080 person-years of follow-up (median=1.9, IQR=1-3.2 years) was 7.3 (95%CI= 5.7-9.4) for ADC [47.6 (95%CI=32.2-70.5) in the first two months] and 2.6 (95%CI= 1.7-4) for NADC. For a 100-cell increase in CD4 at HAART initiation, relative risk of cancer decreased 31% (95%CI 13-45%).
#
Haiti´s data was not included in this analysis.