
Dr Vincent YauWing Lee AsiaPacific Vitreo retina Society Types of Retinal detachment 1 Rhegmatogenous RRD accumulation of subretinal fluid via a retinal break Types of Retinal detachment ID: 934761
Download Presentation The PPT/PDF document "Management of Retinal detachment" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






Slide1
Management ofRetinal detachment
Dr.
Vincent Yau-Wing Lee
Asia-Pacific
Vitreo
-retina Society
Slide2Types of Retinal detachment
1.
Rhegmatogenous
(RRD) accumulation of subretinal fluid via a retinal break
Slide3Types of Retinal detachment2. Tractional (TRD)
vitreous or
fibrovasuclar membrane pulling up the retina, DRM, ROP, Trauma etc
Slide4Types of Retinal detachment3. Exudative
accumulation of
subretinal fluid, with the fluid being derived from blood vessels of the retina, or the choroid, or both Tumor, uveitis, vascular lesion
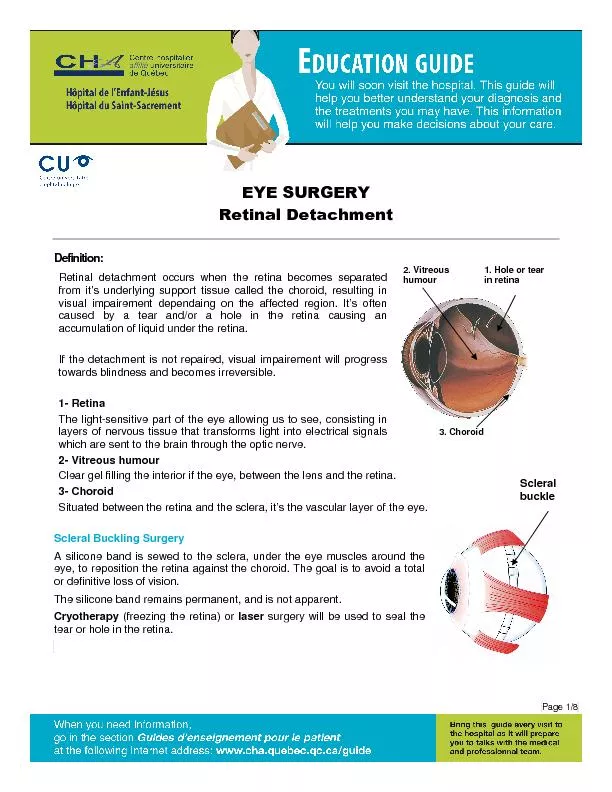
Slide5Rhegmatogenous Retinal detachment (RRD)
Slide6Retina Detachment
Neurosensory retina
Photoreceptors of rods & cones
External limiting membrane
Outer nuclear layer
Outer
plexiform
layer
Inner nuclear layer
Inner
plexiform
layer
Ganglion cell layer
Nerve fiber layer
Internal limiting membrane
Retinal
Pigmented Epithelium (RPE)
Slide7Rhegmatogenous retinal detachment from the Greek word rhegma, which means “a rent”
Slide8How does RRD happen?Understand the normal force keep the retina attached.Understand the relationship between PVD and RDCauses of RD other than PVD
Slide9Normal forces keep the retina attachedhydrostatic pressurephysiologic removal of subretinal fluid by RPE pumpelevated colloid osmotic pressure generated by the high concentration of protein in choroidal tissue fluid
Acid mucopolysaccharide
in the subretinal space (extracellular martix)photoreceptor–retinal pigment epithelium (RPE) interactionmolecular interaction between interdigitating RPE projections and close conformation to the overlying photoreceptors
Slide10Relationship between PVD and RD
Schepens CL. The Vitreous and Vitreoretional Interface. New York, Springer-Verlag, 1987
Slide11Slide12Slide13Consequence of PVDUncomplicated, or
Retinal hole
Vitreous hemorrahage
Retinal tearRetinal detachment
1
2
3
4
Slide14Rhegmatogenous RD (RRD) Causes Posterior vitreous detachmentPeripheral fundus lesion
Myopia
Ocular surgery
– cataract extractionTraumaIntraocular inflammation / infectionSyndromesWagner-Jansen-Stickler SyndromeGoldmann Favre SyndromeMarfan
’s SyndromeHomocystinuria Ehlers-Danlos Syndrome
Slide15Management of RRD
Slide16Pre op exam - Retinal drawing
Slide17The break through of retinal detachment repair
Scleral Buckle (Custodis,1949)
First vitrectomy machine – one port
(Machemer,1970)
Modern 3 port vitrectomy system
(O’Malley,1972)
Slide18Goals of treatment for Retinal DetachmentPreservation of vision. In particular the central vision Relief of inward traction on the retina Closure of all retinal breaksElimination of subretinal fluid
Slide19Relieve traction 1
Slide20Relieve traction 2
Slide21Relieve traction 3
Slide22Modern RD RepairBasic concept:
Main Aim
External steps
Internal steps
Seal retinal break /
Relieve traction
Scleral Buckle
Intraocular gas / silicone oil
Flatten retina
External drainage
Heavy liquid / Gas
fluid exchange
(Internal drainage)
Formation of
Retino-choroidal
adhesion
Cryotherapy
Endo-laser
Slide23Modern RD Repair3 main Types of Surgery:Pneumatic retinopexy
Scleral buckling
Pars plana vitrectomy
Slide24Pneumatic retinopexy
Main Aim
External steps
Internal steps
1. Seal retinal break / Traction relieve
Buckle
Intraocular gas 100%
2. Flatten retina
External drainage
Heavy liquid /
Gas fluid exchange
3. Formation of
Retino-choroidal
adhesion
Cryotherapy
Endolaser
Slide25Pneumatic retinopexyuse of the flotation force and surface tension of an intraocular gas bubble to cause temporary functional closure of the retinal break and displace the break towards the eye ball. successful rate of 63 to 84%
when the retina fail to reattach by pneumatic retinopexy, the patient can still proceed to scleral buckling or pars plana vitrectomy procedures, and the final reattachment rates were shown to be similar.
Advantage: mainly to minimize complications associated with scleral buckling procedure.
Commonest reason for failure in pneumatic retinopexy is missed break intraoperatively or new break formations postoperatively (6-23%). SM Saw. Acta Ophthalmologica Scandinavica, 2006
Slide26Pneumatic retinopexyIndicationretinal break equal to / smaller than 1 clock hours’ sizelocated within the superior 8 clock hours of the peripheral retina
Contraindication
with proliferative retinopathy grade C or above
Aphakic / pseudophakic eye (relative contraindication only)The Retina Detachment Study Group: Pneumatic retinopexy: A multicenter randomized controlled clinical trial comparing pneumatic retinopexy with scleral buckling. Ophthalmology 1989
Slide27Pneumatic retinopexy
Head posture post-operation
for 12 to 18 hours a day for ~ 5 days.
Arrow for proper head posture
Gas bubble as tamponade
Slide28Gas propertyFor Pneumatic retinopexy: 100% gas, 0.3 – 0.5 ml
Slide29Gas dynamicmost rapid rate of volume increase occurs within the first 6 to 8 hours. Sulfur hexafluoride maximally expanded volume by 24 to 48 hours
Perfluoropropane, maximal expansion occurs between 72 to 96 hours
Slide30Practical Tips 1How to achieve a single bubble in the vitreous cavity?Perpendicular needle entryPenetrate the anterior vitreous into mid vitreous
Draw back till needle tip just in vitreous cavity
Position eye ball
– needle at uppermost siteFast but not briskTurn eyeball till needle not at uppermost position
X
1
2
X
Slide31Practical Tips 2The gas is injected as a single bubble by rotating the eye so that the injection site is at the most superior portion of the eye, opposite the tear.
The bubble is rolled under the flap of the tear, keeping the face prone.
The bubble is positioned against flap by rolling the patient.
Slide32Horse shoes Tear with RRD
Pneumatic retinopexy
(Cryotherapy + 0.3ml 100% C3F8 intraocular injection)
Slide332. Scleral buckling surgery
Main Aim
External steps
Internal steps
1. Seal retinal break /Traction relieve
Buckle
Intraocular gas
2. Flatten retina
External drainage
Heavy liquid /
Gas fluid exchange
3. Formation of
Retino-choroidal
adhesion
Cryotherapy
Endolaser
Peritomy
Rectus muscle tagged
Mark break
Cryo
Preplace suture / scleral tunnel
Buckle / encircling
Drainage
Closure
Slide34Normal steps
Slide35Various solid silicone rubber scleral buckling element (MIRA, inc)
Slide36DrainageIndicationDifficulty in localizing breakImmobile retina
Longstanding RD
Inferior RD
IOP rise hazardousTechniqueMost bullous RD area Avoid horizontal meridian/vortex vein
Avoid areas close to breaks
Slide37Special technique“DACE” for very bullous RDDrainage
Air injection
Cryo
Explant
Slide38How to locate a break?? Lincoff rules
Slide39How to locate a break?? Lincoff rules
Slide40How can a buckle work?Decrease the distance between tear and RPE
Change of intraocular fluid current
Relief of vitreous traction (change of vector of force)
Slide41How can encircling work?Support vitreous baseCompartment effectEnhance the buckle effect
Slide42Where to place the encircling band?The greatest diameter of the eye ball – equatorRemember arc length vs cord length
Slide43What determine the height of buckle?The shape of the buckleComposition of the buckle (silicone sponge vs. hard silicone)
Suture placement with respect to the dimensions of the buckle
Suture tension
Distribution of tension from the suture to the buckleIntraocular pressure.
Slide44How does cryotherapy work?Joule-Thomson effectFormation of intracellular ice crystal and mechanical disruption of cell membrane during freezing
Till choroid turn bright orange / retina turn white
Effect in 10-12 days
Slide45Macula on RRD
pre op
Slide46Scleral Buckling + Encircling + Cryotherapy
post op VA = 20/20
Slide473. Pars plana vitrectomy (PPV)
Main Aim
External steps
Internal steps
1. Seal retinal break /Traction relieve
Buckle
Intraocular gas
Silicone oil
2. Flatten retina
External drainage
Heavy liquid /
Gas fluid exchange
3. Formation of
Retino-choroidal
adhesion
Cryotherapy
Endolaser
Slide48Silicone oil property
Slide49TRD (Proliferative DMR) Pre op VA = 20/200
Slide50TRD Post Op
VA = 20/50
Slide51Giant retinal tear with rolled edge
PPV + PFC + laser + PFC / air Exchange + Silicone oil