
Check serum potassium and replace intravenously if value is lt 45mmoll Check serum magnesium and replace intravenously if value is lt 1mmoll Perform a CXR to ensure that a central line if present is not too long and irritating the myocardium ID: 930482
Download Presentation The PPT/PDF document "Ensure AF is not a response to hypovola..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






Slide1
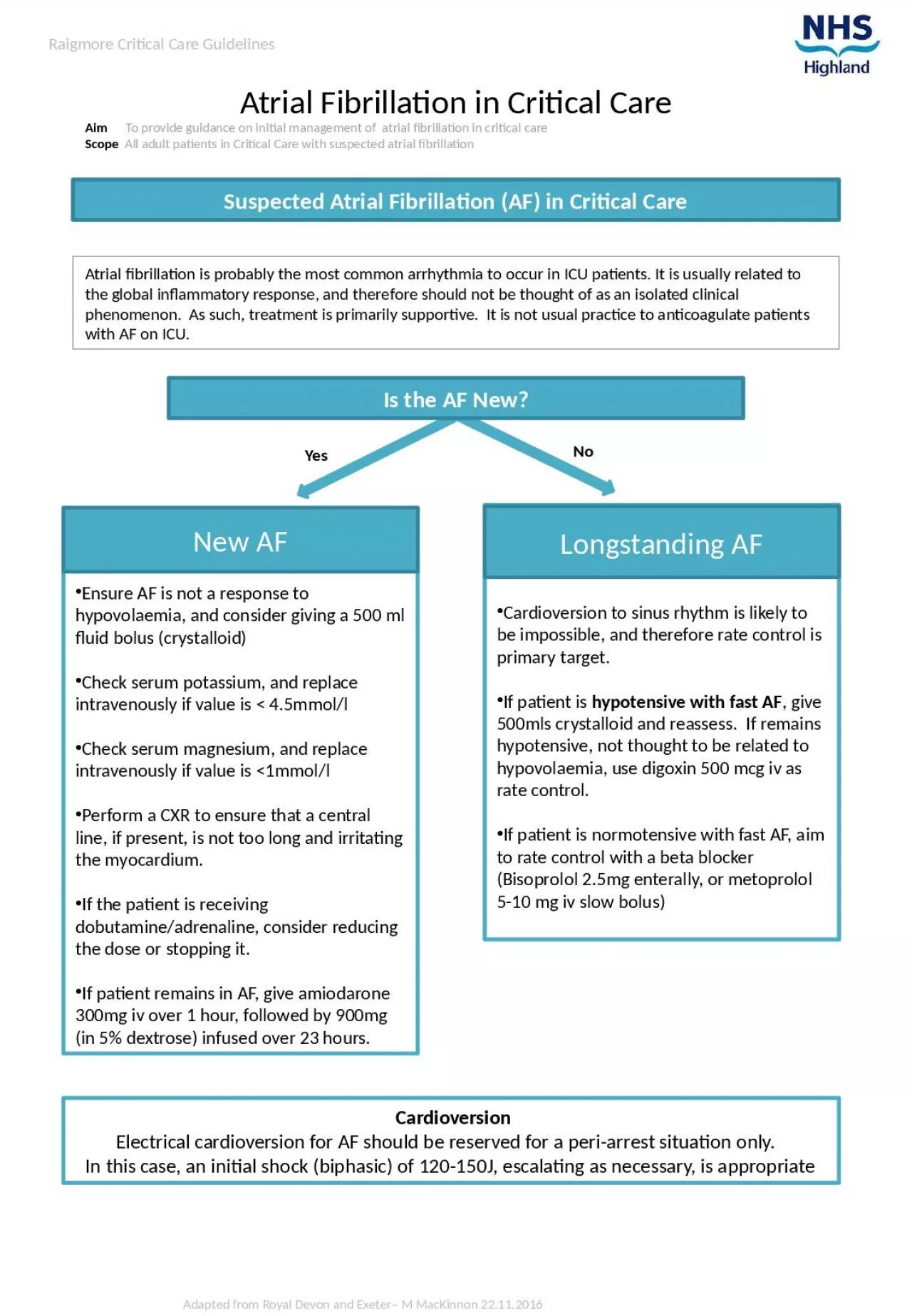
Ensure AF is not a response to hypovolaemia, and consider giving a 500 ml fluid bolus (crystalloid)Check serum potassium, and replace intravenously if value is < 4.5mmol/lCheck serum magnesium, and replace intravenously if value is <1mmol/lPerform a CXR to ensure that a central line, if present, is not too long and irritating the myocardium.If the patient is receiving dobutamine/adrenaline, consider reducing the dose or stopping it.If patient remains in AF, give amiodarone 300mg iv over 1 hour, followed by 900mg (in 5% dextrose) infused over 23 hours.
Cardioversion to sinus rhythm is likely to be impossible, and therefore rate control is primary target.If patient is hypotensive with fast AF, give 500mls crystalloid and reassess. If remains hypotensive, not thought to be related to hypovolaemia, use digoxin 500 mcg iv as rate control.If patient is normotensive with fast AF, aim to rate control with a beta blocker (Bisoprolol 2.5mg enterally, or metoprolol 5-10 mg iv slow bolus)
Suspected Atrial Fibrillation (AF) in Critical Care
CardioversionElectrical cardioversion for AF should be reserved for a peri-arrest situation only. In this case, an initial shock (biphasic) of 120-150J, escalating as necessary, is appropriate
Atrial Fibrillation in Critical Care
Aim To provide guidance on initial management of atrial fibrillation in critical careScope All adult patients in Critical Care with suspected atrial fibrillation
Adapted from Royal Devon and Exeter– M MacKinnon 22.11.2016
Yes
No
Raigmore Critical Care Guidelines
Atrial fibrillation is probably the most common arrhythmia to occur in ICU patients. It is usually related to the global inflammatory response, and therefore should not be thought of as an isolated clinical
phenomenon.
As such, treatment is primarily supportive. It is not usual practice to anticoagulate patients with AF on ICU
.
Is the AF New?
New AF
Longstanding AF