
Mario de los Santos PGY2 Outpatient Report Introduction I Osteoarthritis II Rheumatoid Arthritis III Spondyloarthritis Osteoarthritis History Osteoarthritis often cited as the oldest known disease ID: 775081
Download Presentation The PPT/PDF document " Arthritis and Joint Pain" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
Arthritis and Joint Pain
Mario de los Santos, PGY-2
Outpatient Report
Slide2Introduction
I. Osteoarthritis
II. Rheumatoid Arthritis
III.
Spondyloarthritis
Slide3Osteoarthritis
Slide4History
- Osteoarthritis often cited as the oldest known diseaseEvident in Egyptian mummies and 70 million year-old dinosaur skeletons- Clinically characterized in the late 1700English physican William Heberden Bony outgrowths at DIP joints distinct from gout“Digitorum nodi” Heberden nodes- Treatment Willow bark and leavesSalicylic acidBayer modified to acetylsalicylic acid or aspirin in 1897
Slide5Pathophysiology
- Affects
80% of patients > 55 years or older
and
95% of patients 65 years or older
- Biomechanical process
Joints respond pathologically to mechanical stress
- Acute injury
ACL tear
Repetitive injury (overuse or obesity)
Cartilage injury
Joint laxity
Abnormal joint mechanics
Slide6Risk Factors
- Advancing age
- Obesity
Mechanical, metabolic, or cytokine-driven
Knee OA
- Female gender
- Joint injury
Caused by occupation, repetitive use, or trauma
- Genetic factors
Account for 60-70% of the risk of OA
Slide7Clinical Presentation
- Hallmark features
Pain
Loss of function
- Symptoms worsen with activity and relieved by rest
- Morning stiffness lasting less than 30 minutes
- May recur after periods of inactivity
- Spine
Loss of mobility
Bone spurs
canal stenosis disk bulges nerve root impingement
Slide8Hand Osteoarthritis
- Bony enlargement of the proximal and distal interphalangeal joints Bone spurs- Squaring of the 1st carpometacarpal joint- Clinical manifestationsDecreased range of motionPain that worsens with activity and improves with restSwelling (inflammatory)
Slide9Hand Osteoarthritis
Classic criteria
- Hand
pain (including hand aching or stiffness) plus
at least three
of the following four features:
●Hard tissue enlargement of 2 or more of 10 selected joints. The 10 selected joints are the second and third distal interphalangeal (DIP) joints, the second and third proximal interphalangeal (PIP) joints, and the first carpometacarpal (CMC) of both hands
●Hard enlargement of two or more DIP joints
●Fewer than three swollen metacarpophalangeal (MCP) joints
●Deformity of at least 1 of the 10 selected joints
Slide102012 American College of Rheumatology (ACR) Recommendations
Slide11Role of Physical Therapy
- ACR – Technical Expert Panel- Recommend patient’s with osteoarthritis be evaluated by PT- Assessment of ability to perform ADLs- To evaluate for assistive devices- Instruction in joint protection techniques- Provide thermal agents for relief of pain and stiffness
Slide12Slide13Knee Osteoarthritis
SignsOsteophytesEffusionsCrepitusROM limitationDeformities: Valgus - lateral joint space narrowing (“knock-kneed”)Varus – medial joint space narrowing (“bow-legged”)Cartilage loss medial narrowing more commonBakers cyst – fluctuant swelling along posterior aspect of the knee
Slide14Knee Osteoarthritis
Classic clinical criteria
—
presence of knee
pain plus
at least three
of the following six clinical
characteristics:
●
Greater than 50 years of age
●Morning stiffness for less than 30 minutes
●Crepitus on active motion of the knee
●Bony tenderness
●Bony enlargement
●No palpable warmth
- SN = 95%, SP = 69%
Slide15Slide16Slide17Slide18Hip Osteoarthritis
- Pain around the hipOA of the hipPain referred to the hip from other structures Lumbosacral spine- Groin or buttock painExacerbated by weight-bearing
Slide19Hip Osteoarthritis
Classic Criteria
- Presence
of hip pain plus
at least two
of the following three features:
●Erythrocyte sedimentation rate (ESR) of less than 20 mm/h
●Radiographic osteophytes (femoral or acetabular)
●Joint space narrowing on radiography (superior, axial or medial)
Slide20Slide21Joint Injections
- Use
for joints that cause disproportionate pain or limit function
-
Corticosteroids
Successful injection = 3 months pain relief
Long term risks
= cartilage atrophy
No more than 3 injections per year
-
Hyaluronic Acid
Relief for OA of the knee
Series of 3 weekly injections
Most effective when joint is “dry”
Expensive
Similar pain relief to steroids, last 3-6 months
Slide22Indications for consultation
- If diagnosis
uncertain
rheumatology
- For
assistance with needle aspiration or
injection
rheumatology
or orthopedic surgery
-
S
evere
OA unrelieved by oral, topical, and
intra-articular medications
O
rthopedic consultation for surgical evaluation
Hip and knee replacement surgery
Goal - pain
reduction and function similar to patients without arthritis
Effective
– 90% patient satisfaction
Short term outcomes similar in obese and non-obese patients
Physical rehabilitation
Slide23Slide24Rheumatoid Arthritis
Slide25History
- Pre-Columbian North AmericanSymmetrical polyarticular erosive arthritis reportedin Native American remains – 4500 BC- First modern account in 1800 by French medical student Landré-Beauvais- "emollient pastes were applied, blood was let at the arm and foot, and subsequently baths were given for nearly six months, although they made the condition worse."
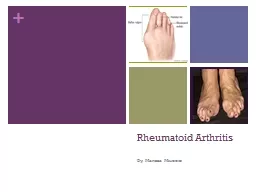
Slide26Rheumatoid Arthritis – Presentation
- Typical Classic RAInsidiousMorning stiffness > 60 minutesPain/Swelling MCP and PIP joints of the fingersInterphalangeal joints of the thumbs and the wristsMTP joints of the toesElbows, shoulders, ankles and kneesSparing of the lumbar spine and DIP joints- Annual incidence = 30 per 100,000 worldwide- Age of onset = 30 to 55 years
Slide27Pathophysiology
- Proinflammatory cytokines – TNF alphaInduce the production of degradative enzymes and promote osteoclast activation cartilage damage and bone erosion
Slide28Presentation
- Initial clinical
p
resentation
Polyarticular
disease with gradual onset
Systemic symptoms: myalgia, fatigue, low-grade fever, weight loss and depression.
- Palindromic rheumatism
Episodic pattern
One to several joints are affected sequentially for hours to days
Alternating symptom-free periods lasting days to months
-
Monoarthritis
Large joints – wrist, knee, shoulder, hip or ankle
Slide29Laboratory Analysis
- Labs
ESR
CRP
Anemia of chronic disease
Thrombocytosis
Hypoalbuminemia
- Synovial fluid analysis
Elevated leukocyte counts with neutrophil predominance
Slide30Serology
-
Rhematoid
Factor - present
in up to 70%
(
sp
= 80%)
Mixed
cryoglobulinemia
(100%)
Sjogren
syndrome (70%)
Systemic lupus erythematosus (20-30%)
Healthy population (up to 10%)
- Anti-
citrullinated
peptide
Specificity = 95%
- ANA
Present in up to 40%
- Absence of anti-CCP and RF does not rule out RA
Slide31Slide32Imaging Studies
- Plain radiographsHands and feet images should be obtained at baseline and at repeated intervalsPeriarticular osteopeniaErosionsSymmetric joint-space narrowing- MRI Can detect bone erosions earlier - UltrasoundDetects synovitisNo established role in diagnosis or prognostication
Slide33Extraarticular Involvement
- Cardiovascular
Premature coronary artery disease
- Musculoskeletal
Low bone mass and fracture
WHO – incorporated RA in the web-based fracture risk calculator (FRAX)
-
Pulmonary
Interstitial
lung disease
- Dermatologic
Felty
syndrome – pancytopenia, splenomegaly and leg ulcers
- Skin
Rheumatoid vasculitis
Rheumatoid nodules
- Ophthalmologic
Scleritis
and scleral ulcers
- Renal
Secondary amyloidosis
Slide34Management
- Aims of treatment:
Eliminate
inflammation
quickly
Preserving function
Maintain remission
Avoiding
joint
injury
- Regular visits
Fatigue, weight loss, morning stiffness, joint pain, functional limitations and acute phase reactants
Radiographic monitoring
Progressive joint damage = insufficient therapeutic regimen
Slide35Management
- NSAIDs
Do not alter disease course
Symptomatic relief
- Corticosteroids
Used to reduce inflammation initially while other agents become effective
High-doses used for extra-articular manifestations
- Disease-Modifying
Antirheumatic
Drugs (DMARDs)
Reduce or block joint damage
Initial choice depends on disease duration, activity and prognosis
Slide36Non-biologic DMARDs
- Methotrexate
Gold standard therapy
Better tolerated, good efficacy, low cost
-
Hydroxychloroquine
, sulfasalazine and minocycline
Relatively short disease duration
L
ow disease activity
N
o evidence of erosive disease
- Combination therapy: sulfasalazine, MTX, and
hydroxychloroquine
Poor prognostic features
Moderate – high level of disease activity
Slide37Biologic DMARDs
- Used when non-biologic DMARDs do not achieve remission
- TNF-alpha inhibitors
Etanercept
(Enbrel)
Infliximab (
Remicade
)
Adalimumab
(
Humira
)
Certolizumab
pegol
(
Cimzia
)
- No clear difference in efficacy
- Combination biologics should be avoided.
- MTX + TNF-alpha inhibitor = further reductions in disease activity
- Rituximab (anti-CD20+)
FDA approved in combination with MTX for TNF-alpha inhibitor non-responders
Slide38Spondyloarthritis
Slide39Ankylosing Spondylitis
- Affects 0.1% of the U.S. population- Male predominance - Peak age of onset is 20-30 years- Association with HLA-B27- Initial pain:Low backButtocksPosterior thighs- Progressive inflammatory back pain and stiffnessBony changes ascend the spine stooped postureLimited mobility of the spine and the chest
Slide40Slide41Psoriatic Arhtritis
- Affects up to 30% of patients with psoriasis- FeaturesEnthesitisDactylitis (sausage digit)Tenosynovitis- Patterns of diseaseArthritis of the distal interphalangeal joints Asymmetric oligoarthritis (<5 joints)Symmetric polyarthritisArthritis mutilansSpondylitis
Slide42Reactive Arthritis
- Post-infectious, aseptic, usually
oligoarticular
and self-limited (6 months)
- Develops days to weeks after infection
- Annual incidence: 30 per 100,000 persons
- 1/3 manifest triad: arthritis, urethritis and conjunctivitis
- Classic pathogens
Campylobacter
Chlamydia trachomatis
Salmonella
Shigella
Yersinia
Slide43Inflammatory Bowel Disease-Associated Arthritis
-
Arthritis is the most common
extraintestinal
manifestation of IBD
Peripheral
Axial
- 50% of patients with IBD develop musculoskeletal symptoms
- Arthritis can develop prior to GI manifestations
- Colonic involvement = higher risk
- Peripheral
arthropathy
Parallels disease activity
-
Spondyloarthropathy
(ankylosing spondylitis,
sacroilitis
)
Does not
parallel disease activity
Slide44References
-
Marc C. Hochberg, Roy D. Altman, et al. American College of Rheumatology 2012 Recommendations for the Use of
Nonpharmacologic
and Pharmacologic Therapies in osteoarthritis of the Hand, Hip, and Knee.
Arthritis Care and Resea
rch 2012; 465-474
- Kenneth C
Kalunian
.
Diagnosis and classification of osteoarthritis
.
In:
UpToDate
, Post TW (Ed),
UpToDate
, Waltham, MA. (Accessed on
January 18 2015.)
-
Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association.
Arthritis Rheum
1986; 29:1039
.
-
Peat G, Thomas E, Duncan R, et al. Estimating the probability of radiographic osteoarthritis in the older patient with knee pain.
Arthritis Rheum
2007; 57:794
.
-
PJW
Venables
, et al.
Clinical manifestations of rheumatoid arthritis
.
In:
UpToDate
, Post TW (Ed),
UpToDate
, Waltham, MA. (Accessed on
January 22, 2015.)
-
Jacoby RK, Jayson MI,
Cosh
JA. Onset, early stages, and prognosis of rheumatoid arthritis: a clinical study of 100 patients with 11-year follow-up.
Br Med J
1973; 2:96
.
-
Zeidler
H, Amor B. The Assessment in
Spondyloarthritis
International Society (ASAS) classification criteria for peripheral
spondyloarthritis
and for
spondyloarthritis
in general: the
spondyloarthritis
concept in progress.
Ann Rheum Dis
2011; 70:1
.
-
Rothfuss
KS,
Stange
EF,
Herrlinger
KR.
Extraintestinal
manifestations and complications in inflammatory bowel diseases.
World J Gastroenterology
2006:12:2819-4831