
Allocation Designs Arzu Kalayci MD Parallel Design Simultaneous treatment and control groups Each person is randomly assigned to one treatment group Randomization removes treatment selection bias and ID: 919304
Download Presentation The PPT/PDF document "Parallel , Crossover, and Group" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
Parallel
, Crossover, and GroupAllocation Designs
Arzu Kalayci, M.D.
Slide2Parallel Design
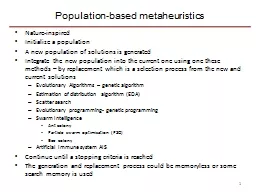
Simultaneous treatment and control groupsEach person is randomly assigned to one treatment groupRandomization removes treatment selection bias and promotes comparability of treatment groupsStatistical comparisons made between treatment groups
Slide3Parallel Design Graph
Current treatmentNew treatment
Improved
Not
improved
Improved
Not
improved
Defined
population
Slide4Crossover Design
Randomization of order in which treatments are receivedAB or BARandomization promotes balance between treatment groups in timing of exposureTesting of both treatments in each patientEach patient serves as his/her own controlVariability reduced because less variability within patient than between patientsFewer patients needed
Slide5Crossover Design Graph
Group 1, Tx A Group 2, Tx AGroup 1, Tx BGroup 2, Tx B
Washout
Slide6Crossover Design: Disadvantages
Treatment can’t have permanent effects or curesPotential carry-over effects of first-period treatment to second periodWashout needs to be long enoughUnequal carry-over effectsTreatment during washoutTest for period by treatment interactions not powerfulDropouts more significantAnalysis may be more difficult
Slide7Crossover Design: Uses
Constant intensity of underlying diseaseChronic diseases—asthma, hypertension, arthritisShort-term treatment effectsRelief of signs or symptoms of diseaseMetabolic, bioavailability, or tolerability studies
Slide8Group Allocation Design
Also known as “cluster randomization”Randomization unit is a group of individuals (community, school, clinic)Individual randomization and intervention is not feasible or is unacceptableTrackingContaminationIf there is a correlation in the responses within a group, design loses some efficiency (more individuals required)
Slide9Group Allocation Design Graph
No interventionIntervention
Improved
Not
improved
Improved
Not
improved
Paired
groups
Slide10Factorial and Large Simple Designs
Slide11Factorial Design
Two interventions tested simultaneously, either as…Economical way to test two treatments simultaneously, orMethod to test for treatment interactionFor testing two treatments simultaneously, assumption is of no interactionTreatments have independent mode of actionMore plausible if different outcome
Slide12Factorial Design Graph
Treatment BTreatment ABoth A and BA but not B
B
but not
A
Neither A nor
B
B,
w/wo A
No B,
w/wo A
No A,
w/wo B
A,
w/wo B
-+
+-
Slide13Factorial Design: Comparisons
Estimation of main effects, if no interaction expectedUse numbers in the margins A vs. no A, regardless of assignment to B B vs. no B, regardless of assignment to AAssessment for interaction Is response in A and no A different among those receiving B or no B? May have limited power to detect interaction
Slide14Factorial Design Graph
Treatment BTreatment ABoth A and BA but not B
B
but not
A
Neither A nor
B
B,
w/wo A
No B,
w/wo A
No A,
w/wo B
A,
w/wo B
-+
+-
Slide15Factorial Design Example: ISIS - 3
International study of Infarct Survival-3Factorial Design: 3x2Aspirin + heparin vs. aspirin alone (antithrombotic)Streptokinase vs tPA vs. APSAC (fibrinolytic)Large, simple trial41,299 patients914 hospitals20 countries
Slide16ISIS- 3 Treatments
ISIS-3 Collaborative Group (1992). Lancet 339: 753-770.
Slide17Large, Simple Design
FeaturesVery large number of patients (many study sites)Broad eligibility criteriaMinimal data collection requirementsRationaleModest benefits require large sample sizesTreatment interactions unlikely, so baseline characteristics and interim response variables are not neededLess precision (more error, increased variance) is tolerated; countered with large numbers
Slide18Large, Simple Design: Requirements
Easily administered interventionShort-term adherenceNo treatment adjustmentNo ongoing monitoring for adverse eventsEasily ascertained outcomeShort-term follow-up?No complex baseline measurementsSimple data are persuasive enough
Slide19ISIS-3 Methods
No baseline form, randomization by phone callTreatment conveniently packagedUse of ancillary treatment not restrictedOne-page form at discharge for in-hospital eventsFollow-up for mortality only, used government records when possibleISIS-3 Collaborative Group (1992). Lancet 339: 753-770.
Slide20Thank you