
StdHighGoldUHCChoicePlusGold01CoverageforEmployeeFamilyPlanTypePOS TheSummaryofBenefitsandCoverageSBCdocumentwillhelpyouchooseahealthplan TheSBCshowsyouhowyouandtheplan wouldsharethecostforco ID: 958976
Download Pdf The PPT/PDF document "StdHighGoldUHCChoicePlusGold01Page1of7Su..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

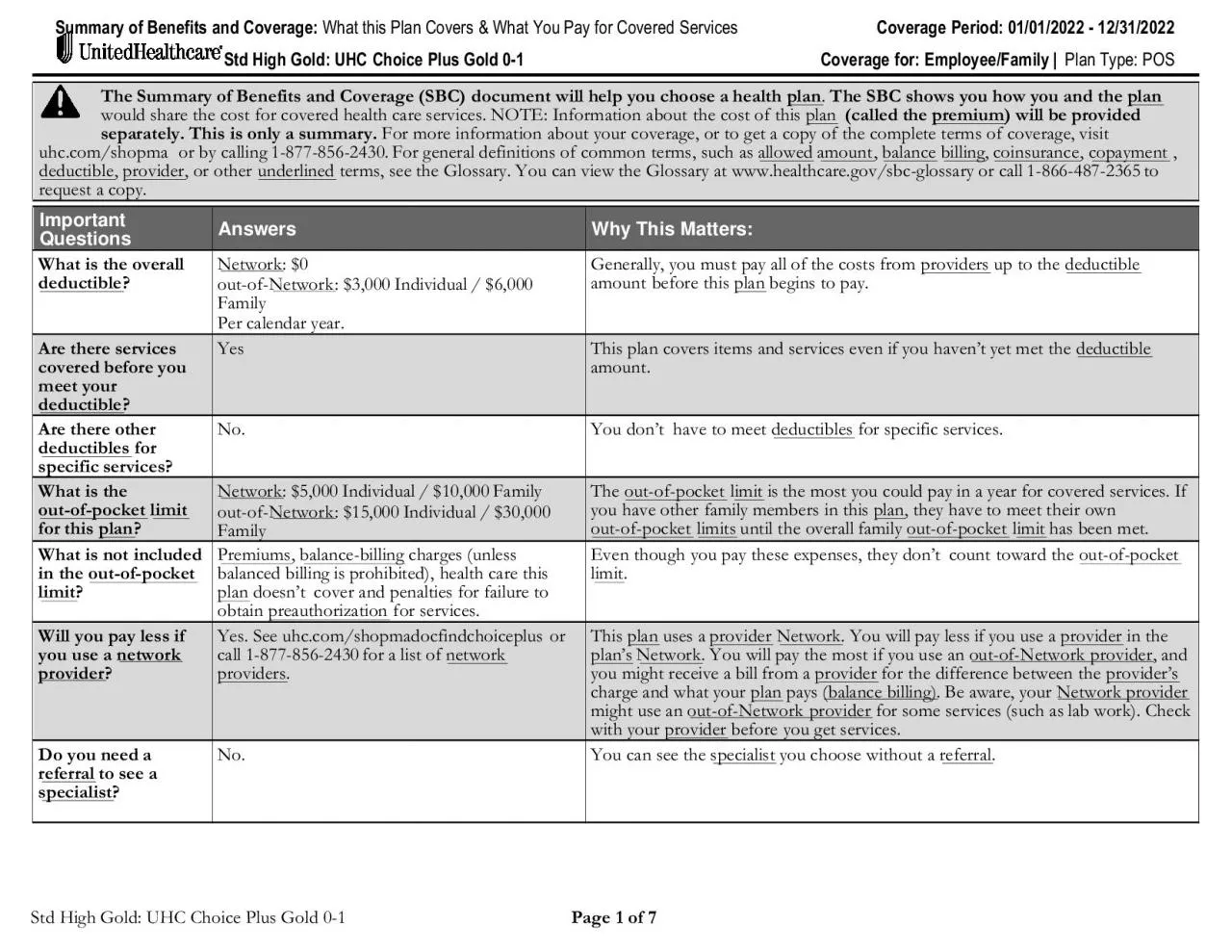
StdHighGold:UHCChoicePlusGold0-1Page1of7SummaryofBenefitsandCoverage:WhatthisPlanCovers&WhatYouPayforCoveredServicesCoveragePeriod:01/01/2022-12/31/2022 StdHighGold:UHCChoicePlusGold0-1Coveragefor:Employee/Family|PlanType:POS TheSummaryofBenefitsandCoverage(SBC)documentwillhelpyouchooseahealthplan .TheSBCshowsyouhowyouandtheplan wouldsharethecostforcoveredhealthcareservices.NOTE:Informationaboutthecostofthisplan (calledthepremium )wil
lbeprovidedseparately.Thisisonlyasummary.Formoreinformationaboutyourcoverage,ortogetacopyofthecompletetermsofcoverage,visituhc.com/shopmaorbycalling1-877-856-2430.Forgeneraldefinitionsofcommonterms,suchasallowed amount billing ,coinsurance ,copayment ,deductible ,provider ,orotherunderlined terms,seetheGlossary.YoucanviewtheGlossaryatwww.healthcare.gov/sbc-glossaryorcall1-866-487-2365torequestacopy. ImportantQuestionsAnswersWhyThisMat
ters: Whatistheoveralldeductible ?Network :$0out-of-Network :$3,000Individual/$6,000FamilyPercalendaryear.Generally,youmust uptothedeductible amountbeforethisplan beginstopay. Arethereservicescoveredbeforeyoumeetyourdeductible ?YesThisplancoversitemsandservicesevenifyouhaven'tyetmetthedeductible amount. Arethereotherdeductibles forspecificservices?No.Youdon'thavetomeetdeductibles forspecificservices. Whatis limit forthisplan ?Network
:$5,000Individual/$10,000Familyout-of-Network :$15,000Individual/$30,000FamilyTheout-of-pocket limit isthemostyoucouldpayinayearforcoveredservices.Ifyouhaveotherfamilymembersinthisplan ,theyhavetomeettheirownout-of-pocket limits untiltheoverallfamilyout-of-pocket limit hasbeenmet. Whatisnotincludedintheout-of-pocket limit ? ,balance-billing charges(unlessbalancedbillingisprohibited),healthcarethisplan doesn'tcoverandpenaltiesforfailur
etoobtainpreauthorization forservices.Eventhoughyoupaytheseexpenses,theydon'tcounttowardtheout-of-pocket limit . Willyoupaylessifyouuseanetwork provider ?Yes.Seeuhc.com/shopmadocfindchoiceplusorcall1-877-856-2430foralistofnetwork providers .Thisplan usesaprovider Network . intheplan's Network .Youwillpaythemostifyouuseanout-of-Networkprovider ,andyoumightreceiveabillfromaprovider forthedifferencebetweentheprovider's chargeandwhatyourp
lan pays(balancebilling) .Beaware,yourNetworkprovider mightuseanout-of-Networkprovider forsomeservices(suchaslabwork).Checkwithyourprovider beforeyougetservices. toseeaspecialist ?No.Youcanseethespecialist youchoosewithoutareferral . Page3of7 MedicalEventServicesYouMayNeedWhatYouWillPay Provider(YouwillpaytheProvider(YouwillpaytheLimitations,Exceptions,&OtherImportant Ifyouneeddrugstotreatyourillnessor Moreinformationaboutprescription
drugcoverageisavailableatwww.uhc.com/shopmad-ruglist202 Tier1-YourLowest-Cost notapply.Retail:$25copay Mail-Order:$50 Deductible notapply.Retail:$25copay Provider meanspharmacyforpurposesofthissection.Retail:Uptoa31daysupply.Mail-Order*:Uptoa90daysupplyor*Preferred90DayRetailNetwork pharmacy.Ifyouuseanout-of-Network pharmacy(includingamailorderpharmacy),youmayberesponsibleforanyamountoverthe amount .Copay isperprescriptionorderuptothe
daysupplylimitlistedYoumayneedtoobtaincertaindrugs,includingcertainspecialty drugs ,fromapharmacydesignatedbyus.Certaindrugsmayhaveapreauthorization requirementormayresultinahighercost.Youmayberequiredtousealower-costdrug(s)priortobenefitsunderyourpolicybeingavailableforcertainprescribeddrugs.Seethewebsitelistedforinformationondrugscoveredbyyour .Notalldrugsarecovered.PrescriptionDrugList(PDL):Advantage.Network:National.Ifadispenseddr
ughasachemicallyequivalentdrug,thecostdifferencebetweendrugsinadditiontoanyapplicablecopay and/orcoinsurance maybeapplied.CertainpreventivemedicationsandTier1contraceptivesarecoveredatNoCharge. Tier2-YourMidrange-Cost notapply.Retail:$50copay Mail-Order:$100 Deductible notapply.Retail:$50copay Tier3-YourMidrange-Cost notapply.Retail:$75copay Mail-Order:$225 Deductible notapply.Retail:$75copay Tier4-AdditionalHigh-CostOptionsNotApplica
bleNotApplicable IfyouhaveoutpatientsurgeryFacilityfee(e.g.,ambulatorysurgerycenter)$500copay visit,deductible doesnotapply20%coinsurance Preauthorization requiredforcertainservicesfor orbenefitreducesto50%ofallowed. Physician/surgeonfeesNoCharge20%coinsurance None IfyouneedmedicalattentionEmergencyroomcare $300copay visit,deductible doesnotapply.$300copay visit,deductible doesnotapply. Emergencymedical transportation NoChargeNoCharge