

Stroke Resources for health Professionals Stroke Foundation Inform Me Page httpsinformmeorgau Includes the living Clinical Management Guidelines which will answer all your questions we dont get to cover today ID: 1044979
Download Presentation The PPT/PDF document "Stroke & TIA SAPMEA PROJECT ECHO | N..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



1. Stroke & TIASAPMEA PROJECT ECHO | Neurology SERIES
2. Stroke Resources for health ProfessionalsStroke Foundation Inform Me Pagehttps://informme.org.au/Includes the ‘living’ Clinical Management Guidelines which will answer all your questions we don’t get to cover today!Available on requestSupport for Country Stroke Services Contact ListSA Stroke Protocols and Pathways document
3. REFERRAL PATHWAYS | OVERVIEW
4. TIA | DiagnosisTIA is defined as focal neurological symptoms due to focal ischaemia that have fully resolvedFacial droopUnilateral limb weaknessDysarthria or dysphasiaUnilateral sensory lossAcute onset vertigoAcute onset ataxiaAcute onset diplopiaMonocular visual lossTransient symptoms usually not due to focal ischaemiaMigraine aura (slow spreading; 10-30min)Generalised weakness/vaguenessSyncopeSeizure activitySymptoms that are persisting or fluctuating should be treated as a stroke → EDHigh risk indicators (i.e. urgent action required)Crescendo TIA (multiple/recurrent episodes over hours to days)or Resolved hemiparesisor >50% stenosis vessel to relevant regionor Current or suspected AFor Current anticoagulant useor High ABCD2 score
5. TIA | ManagementInitial Work UpCT or MRI brain (exclude haemorrhage or confirm stroke)Vessel imaging - CT angiography aortic arch to cerebral vertex MRA (arch to vertex) if CTA contraindicatedCarotid ultrasound (if anterior circulation symptoms and CTA/MRA not available/contraindicated)ECG and Holter monitorCommence secondary preventionReferral for stroke outpatient clinic for urgent (within 1 month) reviewConsider need for driving restriction
6. Acute Stroke Management PathwaysOut of hospital with new onset stroke symptoms - dial 000Country Code Stroke Phone (24/7)Metro (24/7)Patient’s LHN On-Call Stroke Team via switchboardNB: Do not give anticoagulation to a suspected stroke patient prior to imaging (“First do no harm.”)
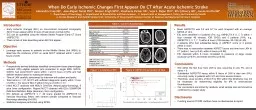
7. Acute stroke management | stroke centreEmergency imaging CT brain, CT angiogram, CT perfusion studyConsider eligibility for hyperacute stroke therapyIV thrombolysis with alteplase or tenecteplaseEndovascular clot retrieval +/- vascular stentingSurgical intervention for ICH or malignant MCA syndromeBlood pressure controlSwallow assessment/NETEarly assessment of rehabilitation needsCase courtesy of Assoc Prof Craig Hacking, Radiopaedia.org, rID: 72596
8. Acute Stroke Management | Stroke CentreWork up for aetiologyCarotid stenosis → consider carotid endarterectomyAtrial fibrillation/flutter → anticoagulation when safe (may need delay in very large stroke)Intracranial atherosclerosis → emerging role for additional therapies beyond the usual (e.g. colchicine)Small vessel/arteriolosclerosisOther rarer causes: thrombophilia, paradoxical embolism (PFO), malignancy, vasculitis, infective endocarditisCase courtesy of Dr Chris O'Donnell, Radiopaedia.org, rID: 42484
9. Post acute care | REHABKey pointsRehab needs assessed and care arranged by acute stroke team prior to dischargeSubacute/older stroke still need stroke management addressed prior to referral to rehabInfo available on HealthPathways SAAllied Health and Nursing > Rehabilitation > Rehabilitation Serviceshttps://southaustralia.communityhealthpathways.org/44724.htmRehabilitation pathwaysStatewide ServicesBrain Injury Services - Brain Injury Rehabilitation Unit (BIRU) & Brain Injury Community & Home (BIRCH)Telerehabilitation ServicesMetropolitan patients (depends on residential address and needs)Private vs publicRehab In The Home (RITH)Day Rehabilitation Services (DRS)Outpatient single discipline (e.g. speech pathology, physio)Private & public optionsCountry patientsSome metro rehab prior to transfer to local servicesRural Rehab Services (NALHN, SALHN, Rural Stroke Centres)Country Health Connect 1800 003 007https://countryhealthconnect.sa.gov.au
10. POST ACUTE CARE | DRIVINGAustroads Fitness to Drive:https://austroads.com.au/publications/assessing-fitness-to-drive‘Appropriate specialist’ in this setting usually refers to a rehabilitation physician rather than a neurologistSpecialist Driving Fitness AssessmentPublic at FMC, QEH and ModburyPrivate options (Calvary, Griffith, OTs)New guidelines due March 2022
11. Secondary preventionLong-term BP management:Target < 140/90 using any agent (best evidence for ACE-I/thiazide) (NB: beta-blockers not first-line unless cardiac disease)Consider more aggressive target (<130 systolic) esp. in haemorrhagic stroke, small vessel disease or diabetesAtrial fibrillationLifelong oral anticoagulation with direct oral anticoagulant (warfarin if other indication (e.g. mech valve) or DOAC contraindication)Under dosing of apixaban is an issueAt least 2 factors before reducing doseAge > 80; weight < 60kg; Cr > 133Left atrial appendage closure only where strong contraindication to anticoagulation existsAnticoagulants usually held until stabilised (4 weeks) in ICH, but may restart sooner 10-14 days in high risk (e.g. mech valve)AntiplateletsSingle agent (aspirin or clopidogrel) in moderate to large strokeAspirin + clopidogrel for 3 weeks then single agent (aspirin or clopidogrel) in high risk TIA and minor strokeLifelong antiplatelet therapy (unless on anticoagulation) in atherosclerosis or arteriolosclerosis related stroke or embolic stroke of undetermined source (ESUS)Treatment for 3-6 months only in arterial dissection strokeCan be restarted once BP controlled and clinically stable in haemorrhagic stroke
12. Secondary preventionCholesterol lowering therapyIf atherosclerosis suspected contributing factor, regardless of lipid levels, high potency statin recommended (e.g. atorvastatin 80mg)Consider omitting if limited life expectancy from other causesTarget LDL < 1.8DiabetesAs per best practice guidelinesLifestyleMediterranean diet or similar (dietitian input helpful)Regular physical exerciseSmoking cessationAlcohol harm reductionOther considerationsDrug-drug interactionsAvoidance of drugs with increased stroke risk (e.g. celecoxib)Medication adherence (e.g. use of aids)Things you don’t need to manage alone!Carotid endarterectomyPatent foramen ovale closureDuration of anticoagulation after cerebral venous sinus thrombosisDecisions about suitability for hormone replacement therapy or COCP in women with stroke
13.
14. OTHER QUESTIONS?Is an abnormal MRI with an old stroke always relevant?It depends. Consider secondary prevention measures. Consider need for additional evaluation (e.g. young patient without risk factors). Consider clinical context (symptoms?).How do we manage cognitive and psychiatric challenges after stroke?Common and can be underappreciated and best management is poorly understoodBrain Injury Rehab services can be helpful in addition to more traditional cognitive and psychiatric management strategies
15. Q&A | EXTRASStroke Triage ToolsROSIER scale (screen for stroke likely dx)Syncope or LOC (less likely)Seizure activity (less likely)New acute onset asymmetrical face or arm or leg weakness, speech disturbance, visual field defect (more likely)ACT-FAST (screen for large vessel occlusion)Arm weaknessR: check speech, L: check neglect/VFOnset < 24hrScreening to exclude stroke mimicsNo known active malignant brain cancer