
Aim To provide a strategy for placement and maintenance of NG tubes Scope All critically ill adult patients Adapted from Queen Alexandra hospital Portsmouth M MacKinnon 30112016 ID: 1009633
Download Presentation The PPT/PDF document "Nasogastric Tubes In ICU" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


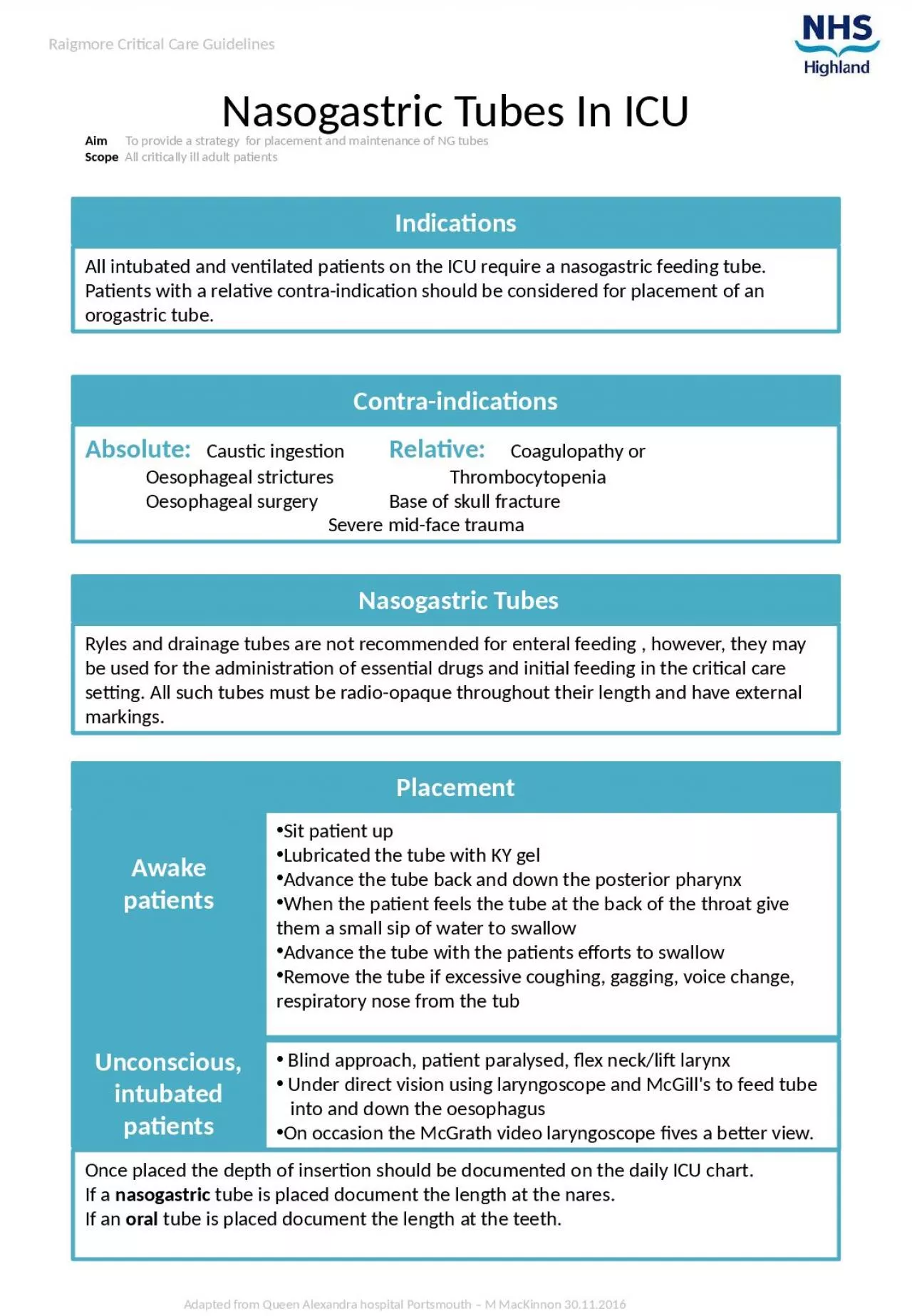
1. Nasogastric Tubes In ICUAim To provide a strategy for placement and maintenance of NG tubes Scope All critically ill adult patientsAdapted from Queen Alexandra hospital Portsmouth – M MacKinnon 30.11.2016Raigmore Critical Care GuidelinesIndicationsPlacementRyles and drainage tubes are not recommended for enteral feeding , however, they may be used for the administration of essential drugs and initial feeding in the critical care setting. All such tubes must be radio-opaque throughout their length and have external markings. Nasogastric TubesAll intubated and ventilated patients on the ICU require a nasogastric feeding tube. Patients with a relative contra-indication should be considered for placement of an orogastric tube.Contra-indicationsAbsolute: Caustic ingestion Relative: Coagulopathy or Oesophageal strictures Thrombocytopenia Oesophageal surgery Base of skull fracture Severe mid-face traumaAwake patientsUnconscious, intubated patientsSit patient upLubricated the tube with KY gelAdvance the tube back and down the posterior pharynxWhen the patient feels the tube at the back of the throat give them a small sip of water to swallowAdvance the tube with the patients efforts to swallowRemove the tube if excessive coughing, gagging, voice change, respiratory nose from the tub Blind approach, patient paralysed, flex neck/lift larynx Under direct vision using laryngoscope and McGill's to feed tube into and down the oesophagusOn occasion the McGrath video laryngoscope fives a better view.Once placed the depth of insertion should be documented on the daily ICU chart.If a nasogastric tube is placed document the length at the nares. If an oral tube is placed document the length at the teeth.
2. Dr C Lee, formatted M MacKinnon 8.4.2017Raigmore Critical Care GuidelinesConfirmation of positionThe nasogastric tube position should be checked radiologically: Following initial insertion Following significant episodes of vomiting, retching or coughing Following evidence of tube displacement (e.g. loose tape or tube appears longer).The nasogastric tube position should be checked clinically: Before administering each feed Before giving medication At least once daily during continuous feeds Ensure patient 30° head up during use Management of NG/OG tubesConfirmation of tube position can only be assured by chest X-ray. Radiological evidence of the NG/OG tube being placed distal to the gastro-oesophageal junction must be confirmed.Landmarks to look for on a chest x-ray: tube descends the thorax in the midline tube bisects the carina (does not follow the outline of the main bronchi) tube crosses the diaphragm in the midlinethe tip sits about 10cm below the diaphragm (gastro-oesophageal junction)Enteral feeding – follow ICU protocolFree drainage-for gastric / enteral ventingMedical patients - decision solely by consultant intensivistSurgical patients – shared decision with surgeonsEnsure one of the intensive care medical team documents in the notes the indications for removal of the NG tube Identify the correct patient, explain and discuss the procedure with the patient. Ensure the patient is sitting upright in the bed Aspirate the gastric contents before removing the tube Instruct the patient to breathe in and hold their breath. This reduces the potential risk of aspiration. Pinch the tube as it is being removed to prevent any contents left in the NG tube draining out into the larynx Examine the skin and mucosa for any sign of trauma and document the procedure and any post removal complications or findings Removal of NG/OG tubes