
Frank A Potestio MSc MD FRCSC Associate Professor NOSM DISCLOSURE No conflict of interest LEARNING OBJECTIVES At the end of this session participants will be able to Classify and quantify the compartments of pelvic organ ID: 921012
Download Presentation The PPT/PDF document "SIMPLIFYING PELVIC ORGAN PROLAPSE" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
SIMPLIFYING PELVIC ORGAN PROLAPSE
Frank A.
Potestio
,
MSc
, MD, FRCSC
Associate Professor NOSM
Slide2DISCLOSURE
No conflict of interest
Slide3LEARNING OBJECTIVES
At the end of this session participants will be able to
Classify and quantify the compartments of pelvic organ
prolapse
(POP)
Plan the evaluation and appropriate referral of women with problematic POP
Select an ongoing maintenance and monitoring plan for women with a
pessary
in place
Slide4CASE STUDY I
A 68
y.o
. female presents with pelvic pressure and a bulging vaginally. She also complains of urinary frequency and urgency, as well as
nocturia
. Examination reveals a stage 3 uterine
prolapse
with a stage 2
cystocoele
. The vagina is also atrophic. Urine culture 2 days ago was negative.
You recommend
Slide5CASE STUDY I
Surgery to correct pelvic organ
prolapse
Use of a
pessary
Vaginal estrogen for
urogenital
atrophy
Medical therapy for overactive bladder
Referral to
urogynecologist
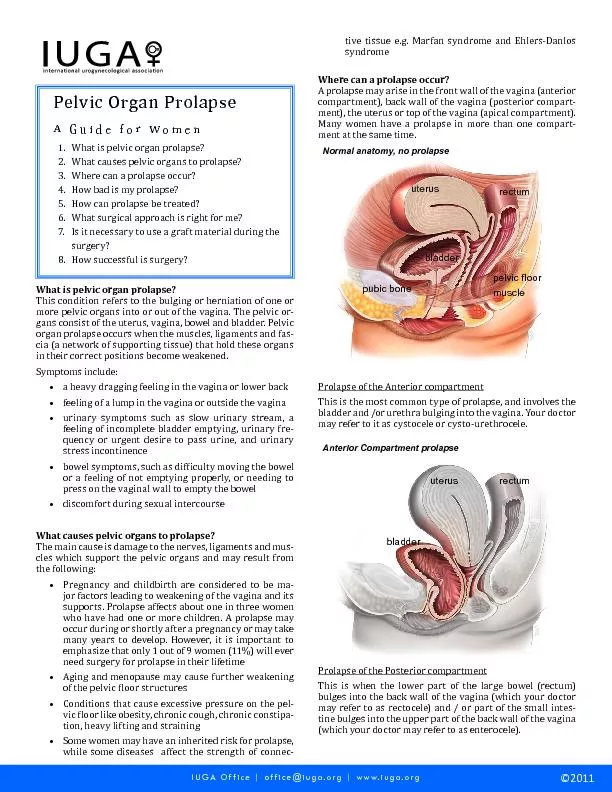
Slide6INTRODUCTION
Pelvic hernia
Affects up to 50 % of
parous
women
10-20 % symptomatic
11 % undergo surgery by age 80
29 – 40 % reoperation within 3 years
Slide7SYMPTOMS OF POP
Bulging
Pelvic pressure
Back ache
Bladder, bowel and sexual dysfunction
Slide8RISK FACTORS
Parity
Intrinsic weakness or atrophy
Obesity
Hysterectomy
Constipation
Connective tissue disorders
Slide9CONFOUNDERS
Urinary incontinence (latent)
Genitourinary syndrome of menopause
Urinary tract infections
Slide10POP CLASSIFICATION
Anterior compartment
cystocoele
Posterior compartment
rectocoele
Apical compartment
uterine, vaginal vault,
enterocoele
anterior > posterior > apical
Slide11BADEN-WALKER HALFWAY SYSTEM
Stage 0: no
prolapse
Stage 1: leading edge > 1cm above hymen
Stage 2: leading edge at level of hymen
Stage 3: leading edge > 1cm beyond hymen
Stage 4: complete
eversion
Slide12POP QUANTIFICATION (POP-Q)
Slide13ANATOMY OF PELVIC SUPPORT
Complex Interaction
Muscles (
levator
ani
)
Fasciae (
urogenital
diaphragm,
endopelvic
)
Ligaments (
uterosacral
, cardinal)
Slide14PATHOPHYSIOLOGY OF POP
Attenuation or stretching of pelvic connective tissue
Site-specific breaks or tears
Anatomical defects in pelvic support
Slide15PRINCIPLES OF SURGERY
Restore normal anatomy & function
Distal
plications
Site–specific repairs
Grafts, meshes bolster defect-specific repairs
Slide16PROSPECT TRIAL (2017)
Synthetic mesh: biological graft: native tissue
Augmentation surgery did not improve outcomes in terms of effectiveness or quality of life
> 1/10 women had a mesh complication
Slide17PESSARY FOR PROLAPSE
First-line treatment
70 – 90 % can be properly fitted
Bulging reduced in 70 – 90 %
Pressure symptoms relieved in 30 – 50 %
20 – 30 % continence rate
Slide18TYPES OF PESSARIES
Support
ring,
Shaatz
, Smith, Hodge,
Gehrung
Space-occupying
cube, donut,
inflatoball
Combination
Gellhorn
Incontinence
Slide19PESSARIES
Slide20PESSARIES
Slide21CHANGES IN POP SYMPTOMS AFTER PESSARY FITTING
Slide22PESSARY CARE
Proper fitting and adequate patient education
Initial follow-up within 2-4 weeks
3 month follow-up if unable to perform self care
6 month or 1 year intervals if no complications arise
Slide23CASE STUDY 2
The 68
y.o
. female who you successfully fitted with a ring
pessary
to manage her symptomatic
cystocoele
and uterine
prolapse
now presents at her 1 year follow-up with vaginal bleeding. She has been compliant with her routine 3 month
pessary
care visits with no concerns.
You recommend
Slide24CASE STUDY 2
Cleaning & reinsertion of
pessary
with reassurance
Removal of
pessary
& examination (including swabs)
Pap smear
Endometrial biopsy
Slide25PESSARY COMPLICATIONS
Erosions (2-9 %)
local pressure leads to
devascularization
Infections (2-3 %)
physiologic response to friction
Rarely major
vesicovaginal
fistulae, bowel fistulae, incarceration
Slide26DISCONTINUATION OF PESSARY
Posterior wall
prolapse
Urinary incontinence
Complications
Slide27SUMMARY
Examination documenting defects in pelvic support (compartment, stage)
Refer women who desire reconstructive surgery that restore normal support and function
Pessaries
should be considered in all women presenting with symptomatic
prolapse
Slide28REFERENCES
Chan M et al., What are the Clinical Factors that are Predictive of Persistent
Pessary
Use at 12 Months? JOGC 2019;41(9):1276-1281.
Larouche
M et al.,
Transvaginal
Mesh Procedures for Pelvic Organ
Prolapse
. JOGC 2017;39(11):1085-1097.
Glazener
C et al. Mesh, Graft or Standard Repair for Women having Primary
Transvaginal
Anterior or Posterior Compartment
Prolapse
Surgery: Two Parallel-Group Multicentre
Randomised
, Controlled Trials (PROSPECT). Lancet 2017; 389(1):381-392.
Magali
R et al., Technical Update on
Pessary
Use. JOGC 2013;35(7):1276-1281.
Beckmann R et al. Pelvic Support Defects, Urinary Incontinence and Urinary Tract Infections. Obstetrics and Gynecology 7
th
edition 2014;30:277-286.
Rock J et al., Surgical / Nonsurgical Correction of Defects in Pelvic Support.
Telinde’s
Operative Gynecology 10
th
ed., 2011.
Slide29Slide30CASE STUDY II
A 88
y.o
. female presents with painful vaginal vault
prolapse
and has tried a number of
pessaries
without success. She had an abdominal hysterectomy 40 years ago. Medical review reveals CAD with persistent angina and moderate COPD from prior smoking. She desires surgical correction if possible and is not sexually active. The most reasonable procedure for her is
Slide31CASE STUDY II
Transabdominal
sacrocolpopexy
Sacrospinous
ligament suspension
LeFort
partial
colpocleisis
Total
colpocleisis
Slide32POP QUANTIFICATION
Slide33POP STAGING
Slide34PELVIC SUPPORT ANATOMY
Slide35PELVIC SUPPORT ANATOMY
Slide36PATHOPHYSIOLOGY (LEVEL I)
Damage to support at or above the
ischial
spines
Involves primarily
uterosacral
ligaments and lesser extent cardinal ligaments
Uterovaginal
prolapse
,
posthysterectomy
vault
prolapse
,
enterocoele
Slide37PATHOPHYSIOLOGY (LEVEL II)
Lateral
midvaginal
support is severed to pelvic sidewall
Involves
endopelvic
fasciae attachment to
arcus
tendineus
fascia
Paravaginal
and
pararectal
defects
Slide38PATHOPHYSIOLOGY (LEVEL III)
Damage to fusion of
urogenital
diaphragm
anteriorly
or proximal perineum
posteriorly
Central defects of fabric of
pubocervical
and
rectovaginal
septa
Cystocoele
,
rectocoele
Slide39PELVIC SUPPORT DISORDERS
Historic: attenuation or stretching of pelvic connective tissue
Recent: site-specific breaks or tears in connective tissue
Identifiable anatomical defects in pelvic support (Levels I,II,III)
Slide40LEVEL OF SUPPORT
Slide41PESSARIES
Slide42PESSARIES
Slide43PREGNANCY
Prolapse
or urinary retention secondary to incarcerated uterus
Decrease preterm birth in parturient women with shortened cervix (< 25 mm)
Use for incontinence not yet described
Slide44PROCEDURES FOR POP
Anterior and posterior
colporrhaphy
McCall
culdoplasty
Sacrospinous
and
uterosacral
ligament vault suspensions
Abdominal / laparoscopic sacral
colpopexy
colpocleisis
Slide45GRAFT USE IN PELVIC FLOOR SURGERY
Synthetic
polypropylene
Xenografts
porcine dermis, porcine small intestine
submucosa
Allografts
cadaveric
Slide46TRANSVAGINAL MESH PROCEDURES
Address specific anatomical defects of the pelvic floor
Maintain durability of repair
Adverse
sequelae
include mesh erosion,
dyspareunia
, pelvic pain, mesh shrinkage, de novo stress incontinence