
tient services Please understand as a link in the Chain of Trust all PHI will remain confidential as mandated by the Treatment Payments and Healthcare Operation Laws mandated by HIPAAReferral for Med ID: 885720
Download Pdf The PPT/PDF document "The information requested above is Prote..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


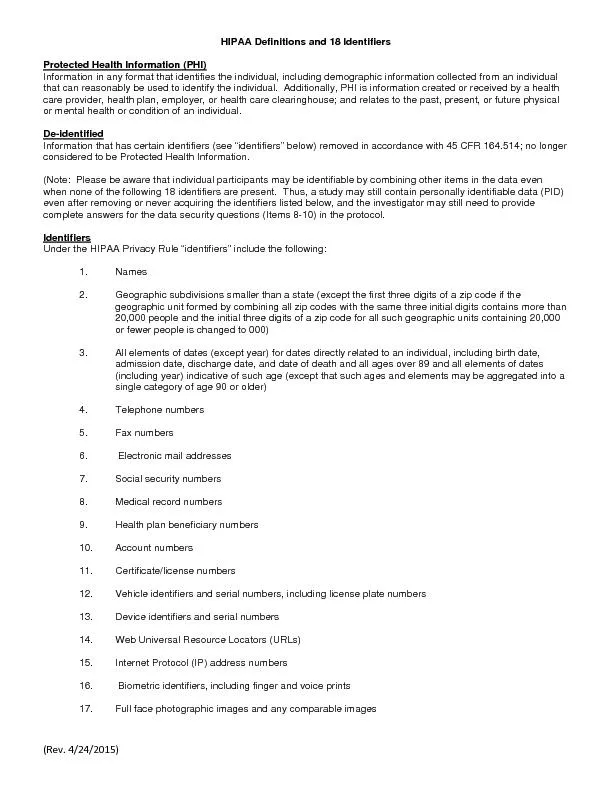


1 The information requested above is Prote
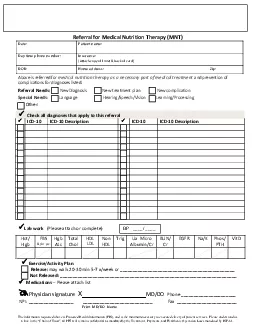
The information requested above is Protected Health Information (PHI), and is the minimum necessary to execute delivery of pa tient services. Pl ease understand as a link in the “Chain of Trust”, all PHI will remain confidential as mandated by the Treatment, Payments, and Healthcare Opera tion Laws mandated by HIPAA. Referral for Medical Nutrition Therapy (MNT) Date: Patient n ame : Day time phone number: Insurance : ( Attach copy of front & back of card ) DOB: Home address: Zip: Above is r eferred for med ica l n utrition t herapy as a necessary part of medical treatment a n d p r evention of c om p lica t i o ns for dia g n os e s l i s te d . Referral Needs: New Dia gno sis N e w trea t ment p lan N ew complicat i on Special Needs : Language Hearing/Speech /Vision Learning/Processing Other : Lab work (Please attach or complete) Hct/ Hgb FBS &/or pc Hgb A1c Total Chol HDL LDL Non HDL Trig Ua Micro Albumin/Cr BUN/ Cr EGFR Na/K Phos/ PTH Vit D Exercise / A ctivity P lan R elease : may walk 20 - 30 min 5 - 7 x/week or __ ____ _ __ ___________ _______ ___________________ Not Released : _______________________________________________________________________ Medications – Please attach list Physician signature X _________________ MD/DO Phone ___________________ ___ NPI: __________________ __________________________ __ Fax _____________ __________ _ Print MD/DO Name Check all diagnoses that apply to this referral ICD - 10 ICD - 10 Description ICD - 10 ICD - 10 Descri ption BP ____/ ____ 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4 4