
lipoproteins particles whose structure includes a core consisting of a droplet of triacylglycerols andor cholesteryl esters a surface monolayer of phospholipid cholesterol amp specific proteins apolipoproteins eg B100 ID: 1000511
Download Presentation The PPT/PDF document "1 Lipoproteins Most lipids are transport..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


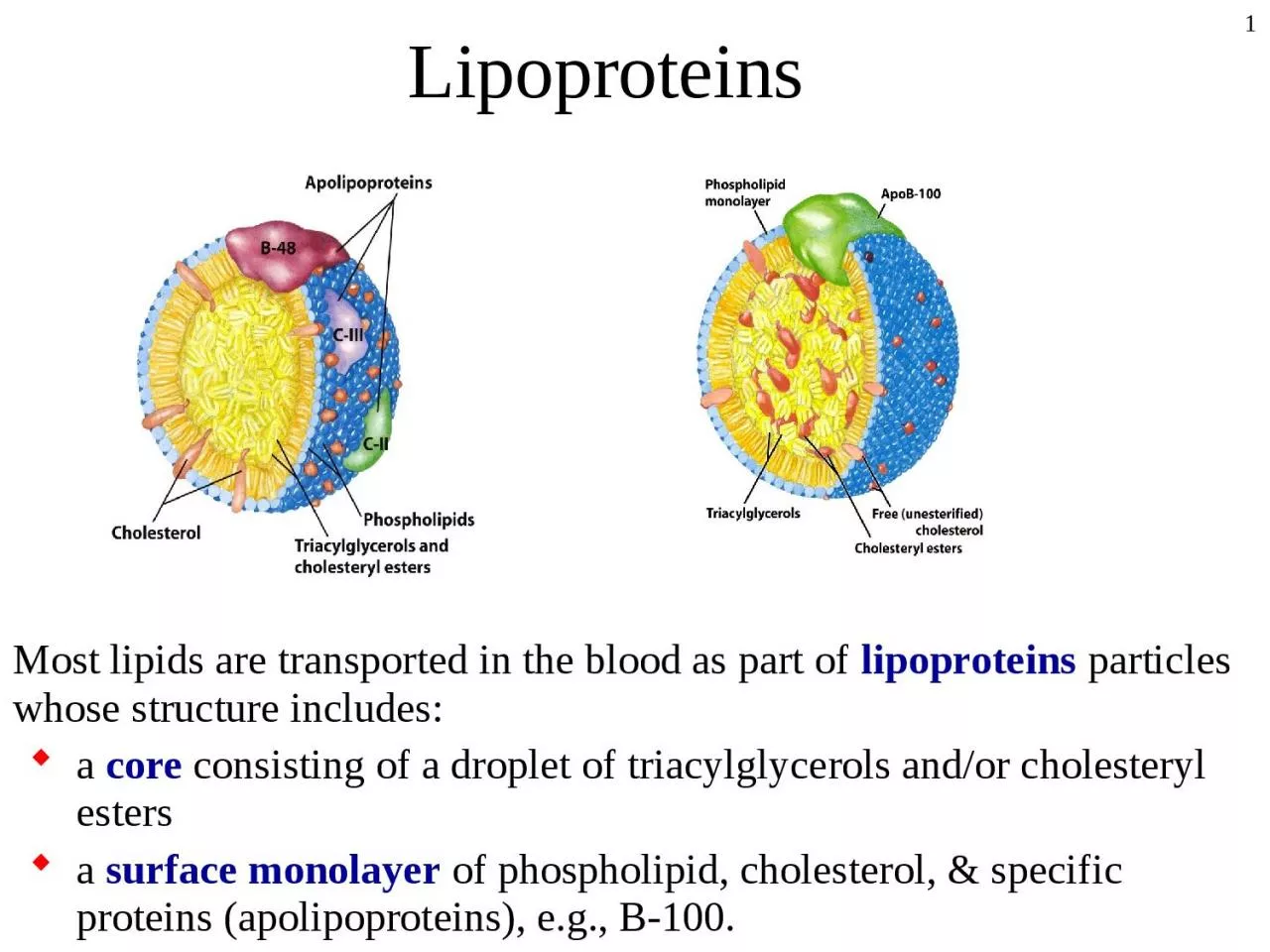
1. 1LipoproteinsMost lipids are transported in the blood as part of lipoproteins particles whose structure includes:a core consisting of a droplet of triacylglycerols and/or cholesteryl estersa surface monolayer of phospholipid, cholesterol, & specific proteins (apolipoproteins), e.g., B-100.
2. 2Lipoprotein classesLipoproteins differ in their contents of proteins and lipids. They are classified based on density. Chylomicron (largest; lowest in density due to high lipid/protein ratio; highest % weight triacylglycerols)VLDL (very low density lipoprotein; 2nd highest in triacylglycerols as % of weight)IDL (intermediate density lipoprotein)LDL (low density lipoprotein, highest in cholesteryl esters as % of weight) HDL (high density lipoprotein; highest in density due to high protein/lipid ratio)
3. 3Images of Lipoprotein particles
4. 40%20%40%60%80%100%Chylo-micronsVLDLLDLHDLLipoprotein TypeCompositionCPTCPTTPCC PTtriacylglycerol (T), cholesterol (C) and protein (P).Composition of major classes of lipoproteins
5. 5Important apoproteinsApoproteinLipoprotein AssociationFunction and CommentsapoA-I , II, and IVChylomicrons, HDLmajor protein of HDL, activates LCATapoB-48Chylomicronsexclusively found in chylomicrons, derived from apoB-100 gene, but lacks the LDL receptor-binding domainapoB-100VLDL, IDL and LDLmajor protein of LDL, binds to LDL receptor; one of the longest proteins in humans- M.W.=513,000apoC-I, II, and IIIChylomicrons, VLDL, IDL and HDLactivates lipoprotein lipase, ApoC-III inhibits lipoprotein lipaseapoE -(multiple isoforms)Chylomicron remnants, VLDL, IDL and HDLbinds to LDL receptor, apoEe-4 allele amplification associated with late-onset Alzheimer's diseaseapoH- at least 19 different alleles; Chylomicronstriacylglycerol metabolism; association with coronary artery disease
6. 6ChylomicronsChylomicrons are assembled in & secreted by the intestinal epithelial cells, transported via the exogenous pathway to deliver dietary cholesterol and triacylglycerols to the body In the bloodstream, chylomicrons acquire apoC-II and apoE from HDLs. Apoprotein CII activates Lipoprotein Lipase (attached to the luminal surface of small blood vessels). Released fatty acids & monoacylglycerols are picked up by tissues as energy sources. During the removal of fatty acids, a substantial portion of phospholipid, apoA and apoC is transferred to HDLs, preventing further degrading of the particle. Chylomicron remnants are taken up by liver cells, via receptor-mediated endocytosis. The process involves recognition of apoprotein E of the chylomicron remnant by receptors on the liver cell surface.
7. 7VLDLThe liver packaged all triacylglycerols available into VLDLs.VLDLs are released into the circulation for delivery to tissues (primarily muscle and adipose tissue) Major lipoproteins are: apoB-100. They acquire apoCs and apoE from circulating HDLsControl of VLDL production:VLDL assembly is dependent on availability of lipids. Availability of apoprotein B-100; regulated transfer of B-100 out of the ER for degradation via the proteasome.
8. 8IDL & LDLIn the circulation VLDLs are converted to LDL through the action of lipoprotein lipaseThe fate of IDLs is either conversion to LDLs or direct uptake by the liver. Major lipoproteins: apoB-100 of LDL and apoE of IDL. Both are recognized by the same receptor: LDL-ReceptorLDLs are the primary plasma carriers of cholesterol for delivery to all tissues.LDL-receptor is a major pharmacological target, and is mediator of most cholesterol-related diseases.
9. 9HDLThe cholesterol esters are scavenged from cell surfaces or transfer to other lipoproteins. HDL may be taken up by liver & degraded. Apoprotein A-1 activates LCAT (Lecithin-Cholesterol Acyl Transferase), which catalyzes synthesis of cholesteryl esters from lecithin. HDL thus transports cholesterol from tissues & other lipoproteins to the liver, which can excrete excess cholesterol as bile acids. High blood levels of HDL (the "good" cholesterol) correlate with low incidence of atherosclerosis.HDL is secreted as a small protein-rich particle by liver and intestine.
10. 10Special Classes of lipidsCholesterol2) Eicosanoids
11. 11Cholesterol HomeostasisCholesterol is an extremely important biological molecule that has roles in membrane structure, and as a precursor for the synthesis of the steroid hormones and bile acids. Sources of cholesterol are either dietary or de novo synthesisSlightly less than half of the cholesterol in the body derives from biosynthesis, mostly in the liver, intestine, adrenal cortex, and reproductive tissuescholesterol (both dietary and synthesized) are transported through the circulation in lipoprotein particles. The same is true of cholesteryl esters (the storage form).
12. 12FATES OF CHOLESTEROLCholesterol cannot be broken down by mammalian cells: Use or LoseUsage: Membrane component, precursor of bile salts, steroid hormones, and vitamin DElimination: Conversion into bile salts (50% of total) or other steroids. Excess dietary cholesterol may also be eliminated via feces or Bacterial reduction to neutral sterols.
13. 13Biosynthesis of CholesterolCholesterol is synthesized by most cells. Synthesis occurs in the cytoplasm and microsomes from the two-carbon acetate group of acetyl-CoA.Synthesis of 1 mole of cholesterol consumes:18 moles of acetyl CoA, 36 moles of ATP, and 16 moles of NADPH.All these elements must be abundant for synthesis to proceedOther biologically essential compounds are also made along this pathway:Dolichol:transports sugars during glycoprotein synthesisPolyisoprenoids:used to tether some proteins to the cell membranecoenzyme Q (ubiquinone)functions in the electron transfer chainCholesterol synthesis has five major steps:
14. 14Stages of cholesterol biosynthesis
15. 15Acetyl-CoA TransportThe acetyl-CoA utilized for cholesterol biosynthesis is derived from citrate of the mitochondria Citrate is transported to the cytoplasm by a specific porterATP-Citrate lyase converts citrate into OAA + Ac-CoAThe reaction catalyzed by malic enzyme generates NADPH, which is required for cholesterol biosynthesis.
16. 16HMG-CoA SynthesisHMG-CoA is formed by condensation of acetyl-CoA & acetoacetyl-CoA, catalyzed by HMG-CoA Synthase.HMG-CoA is the precursor for cholesterol synthesis AND an intermediate of ketone bodies synthesis. The enzymes for ketone body production are located in the mitochondrial matrix. HMG-CoA destined for cholesterol synthesis is made by equivalent, but different, enzymes in the cytosol.
17. 17MITOCHONDRIONFatty acids(2) Acetyl CoA-oxidationAcetoacetyl CoAHMG CoAHMG CoA synthaseThiolaseAcetoacetate-HydroxybutyrateKetone bodies (only synthesized in liver)HMG CoA lyaseoxaloacetateCitrateCitrateAcetoacetyl CoAHMG CoAMevalonateCHOLESTEROLcytoplasmsmoothendoplasmicreticulumHMG CoA reductaseHMG-CoAsynthaseThiolase(2) Acetyl CoA Lyase (requires ATP)OAA malate + NADPH malic enzymeFASTINGFEDHMG-CoA: ketone bodies versus cholesterol
18. 18HMG-CoA ReductionConversion of HMG-CoA to Mevalonate is the rate limiting step, catalyzed by HMG-CoA Reductase Mechanism: carboxyl of HMG is reduced to an aldehyde then to an alcohol via 2-steps reaction using 2 NADPH as reductants. HMG-CoA Reductase is an integral protein of endoplasmic reticulum membranes. Regulation of this enzyme is the primary means for controlling the level of cholesterol biosynthesis. HMG-CoA Reductase is highly regulated enzyme in vivo and is the target of pharmaceutical intervention.
19. 19Short-term regulation:feed-back inhibitionCholesterol acts as a feed-back inhibitor of HMGR; it also induces rapid degradation of the enzyme.Covalent modificationHMG-CoA Reductase is inhibited by phosphorylation, catalyzed by AMP-Dependent Protein Kinase Hormonal regulation via phosphorylation and dephosphorylation (which also regulates fatty acid synthesis and catabolism). Low ATP High AMP active kinase inhibition of HMG-CoA reductase NO cholesterol synthesisBiochemical Regulations of HMG-CoA Reductase
20. 20Long-term regulation:Involves formation and degradation of HMG-CoA Reductase and several other proteins involved in cholesterol homeostasis. Regulated proteolysis of HMG-CoA Reductase: Degradation of HMG-CoA Reductase is stimulated by cholesterol, oxidized derivatives of cholesterol, & mevalonate.Regulated transcription and proteolysis via several transcription factors such as SREBPs (sterol regulatory element binding proteins) that are activated by proteolysis (both the reductase and proteases are regulated)Biochemical Regulations of HMG-CoA Reductase
21. 21Regulation by DrugsDrugs that are competitive inhibitors of HMG-CoA Reductase include various "statin drugs" such as lovastatin (mevacor) and derivatives (e.g., zocor).A portion of each statin is analogous in structure to mevalonate or to the postulated mevaldehyde intermediate.Intermediates of the cholesterol synthesis are involved in growth signal cascades, and thus, statin drugs have been tried as cancer chemotherapies. Statins, as well as inhibitors of enzymes such as Mevolanate Pyrophosphate Decarboxylase and Farnesyl Protein Transferase, have been found in clinical trials to have toxic side effects.
22. 22Cholesterol TransportCholesterol (both external and internal) is transported in the plasma predominantly as cholesterol esters associated with lipoproteins.Free cholesterol is often esterified for the purpose of distribution, storage, or elimination.
23. 23LDL-ReceptorThe LDL receptor is a single-pass transmembrane glycoprotein with a modular design. The LDL-binding domain on the exterior side of the plasma membrane recognizes & binds apoprotein B-100 and E. Binding of receptor with LDL initiates endocytosisThe vesicle then fuses with an endosomal compartment. The LDL receptor was identified by M. Brown & J. Goldstein, who were awarded the Nobel prize.
24. 24LDL-Receptor RegulationRegulation of LDL-receptor involved mostly degradation and Synthesis of the receptor. This process is highly complex involving proteolysis via several transcription factors such as SREBPs Synthesis of LDL receptor is suppressed by high intracellular cholesterol. High cholesterol decreased synthesis of LDL-receptors decreased LDL uptakeDrugs such as Lovastatin, that block cholesterol synthesis by inhibiting HMG-CoA Reductase, cause increased synthesis of LDL receptors.
25. 25Mutations affecting the LDL receptor are associated with the most common form of familial hypercholesterolemia (high blood cholesterol).Cells with defective LDL receptor cannot take up LDL high circulating LDL , high risk of atherosclerosis.Hypercholesterolemias may be the result of genetic defects in apolipoproteins. e.g., familial defective apoprotein B100 Defective ApoB100 impaired binding of LDL to receptors elevated levels of circulating LDL High cholesterol. LDL-Receptor Mutations
26. 26Cholesterol and Heart DiseasesRegulation of cholesterol metabolism is tightly controlled.High cholesterol is:Associated with hardening of arteries and many heart diseasesAppears to coat the arteries Plaque formationResults inIncreased blood pressure due to narrowing of arteries and reducing their ability to stretchClot formation leading to myocardial Infraction and Stroke
27. 27AtherosclerosisVarious factors can initiate formation of a lesion in the endothelium of the arterial lumen.Inflammatory response (cytokines), oxidized lipoproteins, Hypertension, and smoking.Increased permeability of vascular endothelium LDL leak across the endothelium and accumulate in the subendothelial space. High LDL penetration more LDL oxidation cannot bind to LDL receptorMacrophages accumulate at the lesion site. They ingest lipoproteins and appear as “foam cells”. Smooth muscle cells may also migrate into the subendothelial space & become foam cells.As foam cells eventually die, they may release harmful cellular contents that can contribute to rupturing of the plaque and development of blood clots.
28. 28
29. 29Cholecystogram = gall stoneNormal condition: Bile acids, cholesterol and phospholipids are secreted into gallbladder. (bile + cholesterol) = phospholipids soluble cholesterol minimal precipitation of cholesterol in the gallbladder.Under high cholesterol condition:(bile + cholesterol)> phospholipid problems with solubilizing cholesterolcholesterol crystallization in gall bladder plus high bile concentration = gall stone formation (cholesterol-rich stones).Symptoms:Acute abdominal pain.Vomiting after ingesting fatty foods.High Alkaline phosphatase.
30. 30Metabolism of the EicosanoidsThe 20-carbon compounds
31. 31The Eicosanoids The eicosanoids are derivatives of oleic, linoleic, and linolenic acids Stored as C-20 fatty acids on membrane phospholipidsReleased by phospholipase A2 and immediately converted to active “hormone”Eicosanoids come in 3 forms: Eicosatrienoic, Eicosatetraenoic or EicosapentaenoicEach can produce: prostaglandins (PGs), thromboxanes (TXs) and leukotrienes (LTs). All cells except RBC can produce eicosanoids , but historical derivation of their names: Prostaglandins were originally shown to be synthesized in the prostate gland ; thromboxanes from platelets (thrombocytes); leukotrienes from leukocytes
32. 32Physiological EffectsProstaglandins & related compounds are local mediatorsThey are not transported in the blood, so they are not transported to distal sites within the body. They have specific effects close to their site of formation. They are rapidly degraded (few seconds)They act like hormones; profound physiological effects at extremely low concentrations. For example, they mediate:The inflammatory response (Joints, skin, and eye)Production of pain and feverRegulation of blood pressureControl several reproductive functions (labor)Regulation of wake/sleep cycle
33. 33Eicosanoids ReleaseUnsaturated FAs are frequently esterified at OH on C-2 of phospholipids, especially phosphatidylinositol. Released via hydrolysis by Phospholipase A2 or by Phospholipase C and DAG-lipase.There are multiple Phospholipase A2 enzymes, subject to activation via different signal cascades.The inflammatory signal platelet activating factor activates some variants of Phospholipase A2.Corticosteroids are anti-inflammatory because they inhibit Phospholipase A2
34. 34Eicosanoid MetabolismThere are two major pathways of eicosanoid metabolism: Cyclic pathway that leads to production of prostaglandins, prostacyclins, & thromboxanes. Linear pathway that leads to production of various leukotrienes
35. 35Cyclic PathwayPGH2 Synthase catalyzes the first committed stepPGH2 synthase is a heme-containing dioxygenase, bound to ER membranes. (A dioxygenase incorporates O2 into a substrate).PGH2 Synthase exhibits 2 activities: cyclooxygenase & peroxidase. PGH2 Synthase is sometimes referred to as Cyclooxygenase, abbreviated COX. There are multiple forms of COX
36. 36Two isoforms of PGH2 Synthase are designated COX-1 and COX-2 (Cyclooxygenase I & II).COX-1 is constitutively expressed at low levels in many cell types. It is essential for maintaining the integrity of the gastrointestinal epithelium.COX-2 expression is stimulated by growth factors, cytokines, & endotoxins. UP regulation of COX-2 is associated with inflammation and certain inflammatory disease states such as arthritis. Some cancer cells exhibit increased COX-2 expression. Angiogenesis (blood vessel development, essential to tumor growth) requires COX-2.Recent evidence suggests the existence of a third isoform, designated COX-3Isoforms of PGH2 Synthase
37. 37Physiological stimulusclotting, parturition,gastrointestinal and renal protectionCOX-1constitutiveTXA2plateletaggregationProstacyclinendothelium-anticlottingstomach mucosa: H+, HCO3-, mucusPGE2Kidney: arteriolardilation; Na+/H2O excretionA.PGF2parturitionInflammatory stimulus(tissue injury, chronic arthritis)macrophages/other cellsProteasesInflammation, redness,swelling, painB.COX-2induced by cytokines (e.g., TNF)Other inflammatorymediators(histamine, etc)Prostaglandinsespecially PGE2Actions of two known isoforms COX
38. 38Non-steroidal anti-inflammatory drugs (NSAIDs), such as aspirin and derivatives of ibuprofen, inhibit cyclooxygenase activity of PGH2 Synthase; both forms COX I & COX IIThey inhibit formation of prostaglandins involved in fever, pain, & inflammation. They inhibit blood clotting by blocking thromboxane formation in blood platelets.More selective COX-2 inhibitors have been developed, e.g., Celebrex and Vioxx. COX-2 inhibitors are anti-inflammatory & block pain, but are less likely to cause the gastric toxicity. Acetaminophen has little effect on COX-1 or COX-2, and thus lacks anti-inflammatory activity, but might inhibit COX-3. PGH2 Synthase Inhibitors
39. 39NSAIDS
40. 40The Linear PathwayThe 1st step of the Linear Pathway for synthesis of leukotrienes is catalyzed by Lipoxygenase. Mammals have a family of Lipoxygenase enzymes that catalyze oxygenation of various polyunsaturated fatty acid at different sites. Many of the products have signal roles.
41. 415-Lipoxygenase5-Lipoxygenase, in leukocytes, catalyzes arachidonate 5-HPETE (5-hydroperoxy-eicosatetraenoic acid).A non-heme iron is the prosthetic group of Lipoxygenase enzymes. 5-Lipoxygenase requires the membrane protein FLAP (5-lipoxygenase-activating protein) to facilitate interaction between arachidonate with the enzyme. 5-Lipoxygenase, FLAP, and Phospholipase A2 form a complex in association with the nuclear envelope during leukotriene synthesis in leukocytes. (Other types of signal protein complexes associate with the plasma membrane).5-HPETE is then converted to various leukotrienes that induce inflammation and asthmatic constriction of the bronchioles.
42. 42Inhibitors of 5-lipoxygenaseLeukotrienes are synthesized in WBC, mast cells, and a variety of other tissuesThey are the slow-reacting substances of anaphylaxis (allergic reaction, often fatal); far-more potent than histamine.Leukotrienes are extremely potent (10-10 M) in contracting vascular, respiratory, and smooth muscules. Anti-asthma medications include:inhibitors of 5-Lipoxygenase, e.g., Zyflo (zileuton) drugs that interfere with leukotriene-receptor interactions. E.g., Singulair (montelukast) & Accolate (zafirlukast) block binding of leukotrienes to receptors on the plasma membranes of airway smooth muscle cells.