
in Dysarthric Speakers Motor Speech Conference Antwerp University Hospital October 24 2019 Joe Duffy PhD BCNCD Mayo Clinic Rochester MN Overview VP function amp speech Clinical features of VPI ID: 916776
Download Presentation The PPT/PDF document "Treatment of Velopharyngeal Inadequacy" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
Treatment of Velopharyngeal Inadequacy in Dysarthric Speakers
Motor Speech Conference
Antwerp University Hospital
October 24, 2019
Joe Duffy, Ph.D., BC-NCD
Mayo Clinic
Rochester, MN
Slide2OverviewVP function & speechClinical features of VPIManagement issues & principlesTreatments
Medical
Prosthetic
Behavioral
Slide3Velopharyngeal Closure & SpeechClosure is necessary for:All pressure consonants (stops, fricatives, affricates)Acceptable resonance balance on vowels and vocalic consonants (e.g., r, l, w.)
Closure is
inappropriate
for
Nasals (in English, /m/, /n/, /ng/)
VP closure occurs normally as a steady or constant coarticulation in speech, with periodic release from closure for production of nasal consonants
Slide4Velopharyngeal Muscle Functions
Tensor veli palatini
Levator veli palatini
Palatoglossus
Palatopharyngeus
constrictor pharyngeus superior
(from Fritzell 1969)
Slide5Velopharyngeal Movements During Speech4 Patterns
Retraction, elevation & stretch of velum
Mesial movement of lateral pharyngeal walls
Anterior movement of Passevant’s ridge
Circular/sphincteric
superior
lateral
frontal
Slide6Normal
Inadequate
Velopharyngeal Mechanism Function
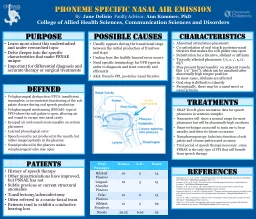
Slide7Primary Speech Consequences of VPI Hypernasality (a vowel phenomenon)“Weak” pressure consonants (reduced perceptual distinctiveness) secondary to audible or inaudible nasal emissionCan place added demands on respiratory & laryngeal functions
Slide8Secondary/Compensatory Speech Consequences of VPI Short breath groups/phrases (air wastage)Reduced loudness (damping effects)Increased subglottal pressure &/or laryngeal hyperadductionFacial grimacing & nares pinching
Glottal stops; pharyngeal fricatives; breathy-hoarse quality; pharyngeal stops; velar fricatives; mid-dorsum palatal stops
Primary & secondary features can reduce intelligibility & efficiency
Slide9Management
Slide10Resonance & VP Speech FunctionCrude assessment of effect of VPI on intelligibility & perhaps other problems – nares occluded vs. unoccludedupright vs. supine
Slide11Focus on Velopharyngeal Function?The pertinent question:If this person was not hypernasal & did not have weak pressure consonant production because of abnormal nasal airflow & VPI, would speech be
More
intelligible
?
More efficient?
Less disabling or handicapping?The answer may be NO for patients with significantly impaired respiratory, phonatory & articulatory abilitiesWhen VP problems outweigh problems in other speech subsystems, focus on VP functions may be appropriate
Slide12Dysarthria Types & VPIType
VP Impairment
Flaccid
May be prominent (Vagus nerve)
Spastic
May be prominent
Ataxic
Normal or intermittent
Hypokinetic
May be prominent, but not common
Hyperkinetic
If evident, intermittent or mild
Unilateral UMN
Uncommon, mild if evident
Mixed
May be prominent, esp. flaccid-spastic
Slide13Other Factors Influencing VP Management DecisionsMedical diagnosis & prognosis Staging SeverityAssociated problemsNonspeech sensorimotor deficitsCognitive-language deficitsEnvironment & communication partners
Motivation, preferences
& needs – Crucial!
The
Health Care System!!!
Slide14Yorkston KM et al.: Evidence-based practice guidelines for dysarthria: Management of velopharyngeal dysfunction. J Med Speech-Lang Pathol, 9:257, 2001.Provides information useful to clinical decision making for surgical, prosthetic & behavioral interventions for VP problems associated with
dysarthria
See Academy of Neurologic Communication Disorders & Sciences website
Slide15Approaches to TreatmentMedicalPharmacologicSurgicalProstheticBehavioral
None are mutually exclusive!
Slide16Approaches to TreatmentMedicalPharmacologicSurgicalProsthetic
Behavioral
Slide17Pharmacologic? No meds that target VPI in any dysarthria type but … Flaccid dysarthria (myasthenia gravis)Mestinon (pyridostigmine bromide) – myasthenia gravisHypokinetic dysarthria (PD)
L-Dopa (levodopa)
Sinemet (carbidopa-levodopa)
Slide18Surgical Pharyngeal flap or sphincter pharyngoplastyGenerally less favorable than prosthetic management; no recent +/- reports Insufficient evidence to permit recommending surgical interventions for VPI in dysarthria
(Yorkston et al., 2001)
Slide19Injection Pharyngoplasty(hyaluronic acid & dextranomer copolymer, calcium hydroxylapatitie, autologous fat) Mostly reported for cleft palate, CA, wind musicians with VPI
Peck et al. (2017)
25 consecutively treated adults with VPI, 52
%
with neuro
etiology (e.g., vagus n; MS, MG, brainstem CVA, myopathy - i.e., flaccid dysarthria) Median follow-up 7.4 months76% required only 1 injection to achieve final resultSig improved resonance, nasalance, & VP gap size Most effective for nonmalignant etiologies & those with good lateral wall motion May hold promise for well-selected dysarthric speakers
Slide20Approaches to TreatmentMedicalPharmacologicSurgicalProsthetic
Behavioral
Slide21Palatal Lift Prostheses
Slide22Palatal Lift Prostheses – evidence compositeEsposito et al. (2000)retrospective study - 25 Ss with ALS 84% had reduced hypernasality76% benefitted for at least 6 months
Yorkston
KM et al
. (2001)
33
articles reviewed Concluded that palatal lift is effective treatment for well-selected individuals with dysarthria
Slide23Palatal Lift Prostheses (cont.) In general, “effective” means increased intelligibilitydecreased hypernasality improved clarity of articulationMost often reported for patients with flaccid >, spastic,
&
mixed
F-S dysarthrias
Some with stable VPI may develop
improved palatal function without lift, perhaps through lift stimulation of neuromuscular responses
Slide24Palatal lift prostheses (cont.)Best candidatesstable or not declining/improving rapidlyless significant/minimal deficits @ other levels
adequate dentition
no significant spasticity (e.g., gag)
motivated, patient, & good self-care ability
Slide25“Minor” Prostheses (nares occlusion)When? Interim while awaiting more substantial interventionRapid changes - decline or improvementPatient uninterested or not candidate for other intervention What?Nasal obturator, nose clip,
one-way
nasal speaking
valves
(Hakel et al., 2004; Suwaki et al., 2008) Manually occluding nares Maybe not for constant use, but helpful for breakdown repairs
Slide26Nares Occlusion
Slide27Approaches to TreatmentMedicalPharmacologicSurgicalProsthetic
Behavioral (modify pattern of speech)
Slide28Principles of Motor Learning “Specificity of training” - Improving speech requires speaking!Training should be as specific as possible to movement patterns, ROM, velocity, force, etc. of ultimate goals of TX“Drill”
–
systematic practice of selected, ordered exercises
Frequent (e.g., twice or more per day)
Frequent brief periods probably better than infrequent lengthy practice
Slide29Behavioral Treatment - VPI Four general behavioral approaches (Yorkston et al., 2001) Techniques focused on nonspeech activities Resistance training during speech Online “instrumental” feedback
Modifying
the pattern of speaking
Limited
evidence. Mixed opinions. Generally felt that dysarthria-based severe & chronic VPI do not benefit from behavioral intervention
Slide30Behavioral Treatment- NonspeechFacilitation techniques - pressure, brushing, icing, stroking, vibratory.Inhibition techniques - prolonged icing, pressure stim., vibration
Motor control tasks
to modify
breath stream (e.g., blowing bubbles, cotton balls, whistles)
Nonspeech strengthening
exercise (blowing, sucking)“The general consensus…these exercises are disappointing and generally ineffective” (Johns, ‘85, p. 158)Nonspeech VP strengthening exercise for dysarthria not justified (Yorkston et al., 2001)
Slide31Resistance Training During Speech Continuous Positive Airway Pressure (CPAP)Positive airflow into nasal cavities through hose & nasal mask assembly Challenges VP muscles to overcome positive pressure (resistance load) to
achieve
VP
closure during
speech
Meets specificity of training motor learning principle Positive effects reported for small # of dysarthric speakers (Cahill et al., 2004; Kuehn et al., 1994; Liss et al., 1994) Success likely reflects careful subject selection & specificity of training speech
Slide32Behavioral Management - Instrumental FeedbackFeedbackMirror at nares; See Scapenasal-flow transducer/nasometernasoendoscope other simple or sophisticated devices that provide feedback about nasal airflow
Mostly testimonial evidence for dysarthrias
Slide33Behavioral Treatment- Instrumental FeedbackVideo game rehab of VP dysfunction (Cler et al., 2017)Feasibility study - at-home case series of
children with
VP
dysfunction
using interactive
video game providing real-time biofeedback from nasal accelerometry to facilitate appropriate nasalizationResults suggest video game–based systems may provide useful platform for real-time feedback of speech nasalizationN = 5 (probably not neuro based)
Slide34Behavioral Treatment- Modifying pattern of speaking (cont.) Active (require learning/practice)Exaggerate jaw movementOverarticulate (“clear speech”)Increase effort/loudness (hypokinetic?)Reduce rate Reduce duration of pressure consonants
Passive
Postural adjustments
(e.g., supine, adjustable bed/wheelchair)
(Yorkston et al., 2001)
Slide35ReferencesDuffy, J.R. (2013) Motor speech disorders: substrates, differential diagnosis, and management (3rd edition), St. Louis: Mosby Elsevier. Guyton
KB et al. Acquired velopharyngeal dysfunction: survey, literature review, and clinical
recommendations
.
Am J Speech-Lang Pathol
; 27: 1572-1597, 2018.Kuehn DP. The development of a new technique for treating hypernasality: CPAP. Am J Speech Lang Pathol. 6:5, 1997.McNeil, M. R. (Ed.) (2009). Clinical Management of Sensorimotor Speech Disorders. (2nd ed.) New York: Thieme Medical Publishers.Peck BW, Baas BS, Cofer SA Injection pharyngoplasty with a hyaluronic acid and dextranomer copolymer to treat velopharyngeal insufficiency in adults. Mayo Clin Proc Inn Qual Out 2017;1(2):176-184.
Yorkston KM et al.: Evidence-based practice guidelines for dysarthria: Management of velopharyngeal dysfunction. J Med Speech-Lang Pathol 9:257, 2001.