
PHG 222 by ADEJARE A A Department of Physiology Faculty of Basic Medical Sciences College of Medicine University of Lagos OUTLINE General organizationfunctional anatomy of the GIT Review of smooth muscle function ID: 909076
Download Presentation The PPT/PDF document "GASTROINTESTINAL TRACT PHYSIOLOGY" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
GASTROINTESTINAL TRACT PHYSIOLOGY
(PHG 222)
by
ADEJARE, A. A.
Department of Physiology
Faculty of Basic Medical Sciences
College of Medicine
University of Lagos
Slide2OUTLINE
General organization/functional anatomy of the GIT
Review of smooth muscle function
GIT motility
GIT secretions and hormones
Digestion and absorption of food substances
Liver and its functions
Nutrition and metabolism
Slide3General organization/functional anatomy of the GIT
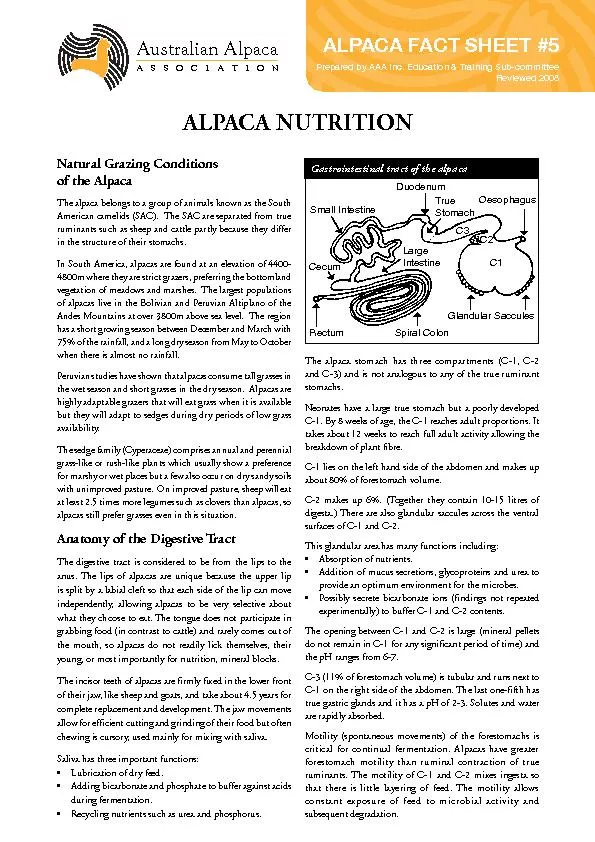
GIT is a
tube that stretches from the mouth to the anus
Function:
serve as a portal for nutrients and water absorption into the body.
GIT: regulatory mechanisms act locally to coordinate the function of the gut
Slide4Alimentary tract
Slide5Physiologic anatomy of the wall
cross section of the intestinal wall:
(1) the
serosa
,
(2) a
longitudinal muscle
layer
,
(3) a
circular muscle layer
,
(4) the
submucosa
,
and
(5) the
mucosa
Slide6Typical cross section of the gut
Slide7Slide8Review of smooth muscle function
Smooth muscle
fibres
are:
Length 200-500
μ
m, diameter 2-10
μ
m
connected with one another through
gap junctions
that allow low-resistance movement
of ions from one muscle cell to the next.
Seperated
by loose connective tissues
each muscle layer functions as a
syncytium
;
Slide9Types of smooth muscle
Multi-unit smooth muscle:
ciliary
muscle, iris muscle,
the
piloerector
muscles.
Unitary or single-unit smooth muscle: contract together as a single unit.
visceral smooth muscle
Slide10GIT smooth muscle
There are two types of electrical waves.
slow waves
and
Spikes
Slow Waves.
Responsible for rhythmical contractions
not action potentials
slow, undulating changes in the resting membrane potential.
Their intensity varies between 5 -15mv
their frequency: 3 to 12
per minute
:
Slide11Slow Waves
RMP: -65 to -45 mV
caused by the
interstitial cells of
Cajal
,
electrical pacemakers
for smooth muscle cells.
Stomach & small intestine: located in the
outer circular muscle layer
Colon:
submucosal
border of the circular muscle layer
The interstitial cells of
Cajal
undergo cyclic changes in membrane potential due to unique ion channels that periodically open and produce inward (pacemaker) currents that may generate slow wave activity.
The slow waves
mainly excite the appearance of intermittent spike potentials,
and the spike potentials in turn actually excite the muscle contraction.
The function of the BER is to
coordinate peristaltic and other motor activity
Slide12Slow waves and spikes
Slide13Spike Potentials
Spike Potentials.
are
true action potentials.
They occur when the RMP becomes more positive than about -40 millivolts
The higher the slow wave potential rises, the greater the frequency of the spike potentials,
between 1 and 10 spikes per second.
The spike potentials last longer
The AP is caused by calcium and sodium ions moving thro
calcium-sodium channels
. K+ for repolarization
These channels are much
slower to open and close
than are the rapid sodium channels of large nerve fibers.
accounts for the
long duration of the AP
.
causes the intestinal muscle fibers to
contract
Slide14Factors that depolarize the membrane
(1)
stretching
of the muscle,
(2) stimulation by
ach
(3) stimulation by
parasympathetic nerves
and
(4) stimulation by
GI
hormones
.
Important factors that hyperpolarize the membrane
and make the muscle fibers less excitable—are
(1) the effect of
norepinephrine
or
epinephrine
(2) stimulation of the sympathetic nerves
Slide15Tonic Contraction of Some Gastrointestinal Smooth Muscle.
Tonic contraction is caused by
continuous repetitive spike potentials—the greater the frequency, the greater the degree of contraction.
hormones
continuous entry of
Ca2+
into the cell
Slide16GIT MOTILITY
Ingestion of food is determined by
Hunger: intrinsic desire for food
Appetite: desire for a particular type of food
Mechanics of ingestion
1. mastication (chewing)
2. swallowing
Slide17Mastication
Chewing
breaks up large food particles and mixes the food with the secretions of the salivary glands.
chewing process is caused by a
chewing reflex
,
The
presence of a bolus of food
in the mouth
first initiates
reflex inhibition
of the muscles of mastication: lower jaw drops.
initiates a
stretch reflex
of the jaw muscles that leads to
rebound
contraction.
This automatically raises the jaw to cause
closure of the teeth
and
compresses the bolus again against the linings of the mouth,
which inhibits the jaw muscles once
again
,
allowing the jaw to drop and rebound another time
Slide18I
mportance
Chewing is important
for
breaking the food
.
chewing aids the digestion increases
surface area
exposed to the digestive secretions.
prevents excoriation of the
GIT
and
increases the ease with which food is
emptied from the stomach into the small intestine
Slide19Regulation
Most of the muscles of chewing are innervated by the motor branch of the
fifth cranial nerve, and the chewing process is controlled by
nuclei in the brain stem
:
Stimulation of specific reticular areas in the brain stem taste centers will
cause rhythmical chewing movements.
stimulation of areas in the
hypothalamus
,
amygdala
the cerebral cortex
Slide20Deglutition
Swallowing can be divided into
a
voluntary stage
, which initiates the swallowing process;
a
pharyngeal stage
, constitutes
passage of food through the pharynx into the
esophagus; and
an
esophageal stage
, transports food from the pharynx to
the stomach.
Slide21Voluntary Stage of Swallowing.
When the food is ready for swallowing, it is “voluntarily” squeezed or rolled posteriorly
into the pharynx by pressure of the tongue
upward and backward against the palate
Slide22Swallowing mechanism
Slide23Pharyngeal Stage of Swallowing.
As the food enters the pharynx, it stimulates
epithelial swallowing receptor areas
and impulses from these pass to the brain stem to initiate a series of automatic pharyngeal muscle contractions as follows:
1. The soft palate is pulled upward to
close the posterior nares
2. The
palatopharyngeal
folds approximate each other.
3. The vocal cords
a
re strongly approximated.
These cause
epiglottis to swing backward over the opening of the larynx
: to prevent passage of food into the
trachea
.
Slide24Stages of deglutition
Slide254. The upward movement of the larynx also
enlarges the opening to the esophagus,
upper esophageal sphincter
relaxes
.
5. The pharynx contracts,
a fast peristaltic wave initiated by the nervous system of the pharynx forces the bolus of food into the upper esophagus which propels the food by peristalsis into the esophagus.
Slide26Slide27Reflex
inhibition:
The swallowing center specifically
inhibits the respiratory center of the medulla during
this time, halting respiration at any point in its cycle to
allow swallowing to proceed.
Slide28Esophageal Stage of Swallowing.
Esophagus
functions to conduct food from the pharynx to the stomach,
exhibits two types of peristaltic movements:
Primary peristalsis
:
continuation of the peristaltic wave that begins in the pharynx 8 to 10 seconds.
S
econdary
peristaltis
:
results from distention of the esophagus itself by the retained food.
Slide29Peristalsis
Slide30Regulation
The musculature of the
pharyngeal wall and upper third of the esophagus
is controlled by
skeletal nerve impulses from the glossopharyngeal and
vagus
nerves
.
In the lower two thirds of the esophagus, the musculature is
smooth muscle
, but this portion of
the esophagus is also strongly controlled by the
vagus
nerves
acting through connections with the esophageal
myenteric
nervous system.
Slide31Function of the Lower Esophageal Sphincter
remains
tonically
constricted
“
receptive relaxation
” for easy propulsion of the swallowed food
into the stomach.
prevent significant reflux of stomach contents into the esophagus
except under very abnormal conditions.
Additional Prevention of Esophageal Reflux by
Valvelike
Closure of the Distal End of the Esophagus.
Slide32LES
Slide33APPLIED PHYSIOLOGY
1. Achalasia: failure of the esophagus to relax
due to
increased resting LES tone
and incomplete relaxation on
swallowing
Treatment:
pneumatic dilation of the
sphincter
incision
of the esophageal muscle (
myotomy
)
Use of
botulinum
toxin to inhibit further Ach release
Slide342.
Gastroesophageal
reflux
disease (GERD): due to LES incompetence
There is
reflux of acid gastric contents into the esophagus
effects: heartburn, esophagitis, ulceration
Treatment: omeprazole, surgery
Slide35Gastric motility
Anatomical division of the stomach
Anatomically, the stomach is usually divided
into two major parts:
(1) the
body
and
(2) the
antrum
.
Physiologically, it is more appropriately divided into
(1) the “
orad
” portion: the first two
thirds of the body, and
(2) the “
caudad
”
portion:the remainder of the body plus the antrum.
Slide36Physiologic anatomy
Slide37Motor Functions of the Stomach
threefold:
storage
of large quantities of food
mixing
of this food with gastric secretions until it forms a semifluid mixture called
chyme
; and
slow emptying
of the
chyme
from the stomach into the small intestine
Slide38Storage Function of the Stomach
Food is
temporarily stored
in the stomach
ff
receptive relaxation
a “
vagovagal
reflex
” from the stomach to the brain
stem and then back to the stomach
reduces the tone
in the muscular wall of the body of the stomach (0.8 to 1.5 liters)
Slide39Mixing function of the stomach
As long as food is in the stomach, weak peristaltic
constrictor waves
, called
mixing waves
, begin in the
mid- to upper portions
of the stomach wall and move toward the
antrum
about once every 15 to 20 seconds.
These waves are initiated by the gut wall
basic electrical rhythm
, consisting of electrical “slow waves” that occur spontaneously in the stomach wall.
Slide40Stomach emptying- 3
rd
fxn
promoted by intense peristaltic ring-like
contractions in the stomach
antrum
50-70 cmH
2
O pressure
each strong
peristaltic wave
forces up to several milliliters of
chyme
into the
duodenum
“pyloric pump.”
The pyloric sphinter regulates flow into the duodenum
Slide41Regulation of stomach emptying
Gastric Factors That Promote Emptying
Increased
food volume
in the stomach promotes increased emptying
from the stomach.
Increased production of
gastrin from
antral
mucosa
caused by
stomach wall stretch and the presence
digestive products of meat
Fat> protein>CHO
Slide42Regulation (
contd
)
Duodenal Factors
1.
Enterogastric
Inhibitory Reflexes: inhibit pyloric pump, increase tone of pyloric sphincter
(1) directly from the duodenum to the stomach through the enteric nervous system in the gut wall,
(2) through extrinsic nerves that go to the
prevertebral
sympathetic ganglia and then back through inhibitory sympathetic nerve fibers to the stomach, and
(3) probably to a slight extent through the
vagus
nerves
Slide43The
enterogastric
inhibitory reflexes are stimulated by
1. distention of the duodenum
2. presence of irritation of the duodenal mucosa
3. acidity of the duodenal
chyme
(< 3.5 - 4)
4. osmolality of the
chyme
5. presence of breakdown products of proteins and fats
Slide44Duodenal Factors That Inhibit Stomach Emptying
2. Hormonal feedback from the duodenum: stimulated by
presence of fat
cholecystokinin (CCK) from jejunum mucosa
Secretin from duodenal mucosa
Gastric inhibitory peptide (GIP) from duodenum and jejunum
Slide45APPLIED PHYSIO
Vomiting:
starts
with salivation and the sensation of
nausea
Reverse peristalsis empties material from the upper part of the small intestine into the stomach.
The
glottis closes, preventing aspiration of vomitus into the trachea.
The
breath is held in mid inspiration.
The
muscles of the abdominal wall contract, and because the chest is held in a fixed position, the contraction increases intra-abdominal pressure.
The
lower esophageal sphincter and the esophagus relax, and the gastric contents are ejected.
Slide46Vomiting pathways
Slide47Intestinal motility
can be divided into
mixing contractions
and
Propulsive contractions
.
mixing
contractions
:
stretching of the intestinal wall
elicits localized concentric contractions.
The contractions cause “
segmentation
” of the small intestine
Slide48Contractions in the small intestine
Slide49The maximum frequency of the
segmentation contractions
in the small intestine is determined by the
frequency of
electrical slow waves
in the intestinal wall
12 contractions/minute in the duodenum/jejunum
8-9
contractions/minute
in
the ileum
Slide50Propulsive contractions
1. peristaltic waves from pylorus to
ileocaecal
valve (3-5 hours, peristaltic rush in
diarrhoea
/ protective):
Control:
Presence of meal
Gastroenteric
reflex
Gastrin
CCK increase
Insulin
Motilin
Serotonin
Secretin
Glucagon decrease
Slide51On reaching the
ileocecal
valve, the
chyme
is sometimes blocked for several
hours until the person eats another meal; at that time,
a
gastroileal
reflex intensifies peristalsis in the ileum
and forces the remaining
chyme
through the
ileocecal
valve into the cecum of the large intestine
Slide52Ileocecal
valve
Slide53Function of
ileocecal
valve
Prevent
backflow of fecal contents from the colon into the small intestine
Has a thickened part,
ileocecal
sphincter which
slows emptying of
ileal
contents into
the cecum
Control
:
distension of cecum increases contraction,
irritation in the cecum delays emptying from ileum
Slide54Colonic motility
The
principal functions
of the colon are
(1) absorption of water and electrolytes from the
chyme
to form solid feces and
(2) storage of fecal matter until it can be expelled.
Slide55Colonic motility
mixing movements
There is combined
contractions of the circular and longitudinal strips of
muscle -
haustrations
.
Haustrations
move slowly to the anus during contraction
propulsive
movements
(8-15hrs)
Also called mass movements
Results from
haustral
contractions
15 minutes after taking breakfast
Slide56Regulation of mass movement
Gastrocolic
reflex
Duodenocolic
reflex. Both under ANS control
Irritation in the colon
eg
in ulcerative colitis
Applied
Physio
Constipation:
refers to a pathological decrease in bowel
movements
Symptoms:
slight
anorexia
mild
abdominal discomfort
distention
Slide57Defecation
Occurs
w
hen a mass movement forces
feces into the rectum
There is reflex contraction of the rectum and
Relaxation of the anal sphincters
Continual dribble of fecal matter through the anus is prevented by tonic constriction of
(1) an
internal anal sphincter
of smooth muscle and
(2) an
external anal sphincter
, composed of striated voluntary muscle that both surrounds the internal sphincter and extends distal to it.
Slide58Control
The external sphincter is controlled by the
pudendal
nerve
, which is part of the somatic nervous system and therefore is under
voluntary
,
conscious control
; subconsciously, the external sphincter is usually kept
continuously constricted
unless conscious signals inhibit the constriction.
Slide59Defecation Reflexes (intrinsic reflex)
Slide60This process is usually fortified by a parasympathetic defecation reflex
1
2
3
4
4
4
4
Slide61Parasympathetic defecation reflex
Slide62Distention of the stomach by food initiates contractions of the rectum and, frequently, a desire to defecate. The response is called the
gastrocolic
reflex
.
Because
of the response, defecation after meals is the rule in children. In adults, habit and cultural factors play a large role in determining when defecation occurs.