
18 th Annual Primary Care and Sports Medicine Symposium January 26 th 2018 Andy Davis MSPT LAT Sport and Spine Clinic of Weston Disclosure No conflict of interest or company affiliation for this presentation ID: 760833
Download Presentation The PPT/PDF document "Running Injuries of the Foot and Ankle" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
Running Injuries of the Foot and Ankle
18th Annual Primary Care and Sports Medicine SymposiumJanuary 26th, 2018Andy Davis MSPT, LATSport and Spine Clinic of Weston
Slide2Disclosure
No conflict of interest or company affiliation for this presentation.
Slide3Running
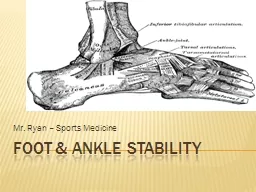
Slide4Anatomy
Slide5Foot and Ankle Injuries
Tendonopathies (Achilles and Posterior Tibialis TendonPlantar FascitisAnkle SprainsFoot fracturesNerve Conditions
Slide6Achilles Tendonapthy
Is the largest tendon of the body and connects the
soleus
, medial and lateral
gastrocnemius
to the
calcaneus
.
Most common sites of injury are at the
midportion
(2-6 cm proximal to the insertion) and at the insertion spot specifically
Prevalence in distance runners has been reported at 5-18% of the total injuries in runners
Slide7Achilles Tendonopathy
Etiology is
multifactorial
Intrinsic factors (tendon
vascularity
, age, gender, body weight, muscle weakness, ROM, lower limb misalignment)
Extrinsic factors (training errors, running technique, footwear, running surface)
Biomechanical variable – hip strength and decreased neuromuscular control of gluteus
medius
and
maximus
(
Creaby
et al, 2017, Am College of Sports Med)
Slide8Achilles Presentation
Mean age 30-50 and more common in malesDecreased PF strengthDecreased PF endurancePain with increased loading walking down stairsTendon thickening/swellingDecreased dorsiflexion ROM (Tenforde et al, 2016, Phys Med Rehabil Clin N Am) (Rabin et al, 2014, J Foot Ankle Research)
Slide9Achilles
Mid –Portion: Pain with direct pressure over the distal third of the achilles (within 2-6 cm of insertion)Insertional: Pain with direct palpation along the medial/lateral aspect of posterior calcaneus. Longer recovery time
Slide10Achilles Tendonopathy (AT)
Runners with
insertional
achilles
tendonopathy
use a greater range of DF
vs
normals
– correlates to increased
symptom
severity
(
Chimenti
et al, 2016,
Orth
Sports Phys
Ther
)
Individuals with AT, had increased DF position with hopping – creating an increase in stretch.
Soleus
activity is reduced
(
Debenham
et al, 2016 J
Sci
Med Sport)
Hip neuromuscular control is altered in runners with AT, specifically gluteus
medius
(
Creaby
M, et al 2017 Am Col Sports Med)
(Kim S, Yu J, 2015 J Sports Science and Med)
(Smith M, et al, 2014 Med and Science Sport and
Exericse
)
Slide11Achilles Treatment
Strong evidence for eccentric strengthening to promote healing in
tendonopathies
as well as strengthening of
soleus
muscle with bent leg exercises.
Pain monitoring – utilizing the visual analog pain scale to give reference point for the patient and patient education
(
Sibernagel
, JOSPT 2015)
Tendon Load Management – avoid hills and reduce the running volume, may have to cross train. Isometric exercises moving into heavy slow resistance.
(
Kountaris
and Cook 2007, Best
Prac
Res
Clin
Rheumatiol
) (Cook and
Purdam
2009, Br J Sports Med)
Slide12Running Mechanics and AT
Pain is usually at propulsive phase of stance, generally not at loading responseWith excessive DF at midstance, causes increase in wrapping or wringing out before the concentric contraction. If the pain is more at the medial insertion point, check for a higher rate of pronation during contactReduce the DF angle – increase cadence Stretching ?? At end range getting tendon wringing out – increased compression.
Slide13Posterior Tibial Tendon Dysfunction
Runs from deep posterior compartment of the leg to insert at the navicular, middle cuneiform, second through fourth metatarsals
Slide14Posterior Tibialis Tendon
Functions as a shock absorber at heel strike,
invertor
of the foot, functions eccentrically from heel strike to
midstance
where it helps stabilize the foot, and aids in force generation at heel lift and toe off
Usually a slow progressive presentation
Swelling and tenderness are commonly present. Need to palpate/inspect the proximal aspect of the muscle
Pain and or weakness with resisted inversion of a plantar flexed foot
(Kindred J, et al 2011 Current Sports Medicine Reports)
(
Tenforde
A, et al 2016 Phys Med
Rehabil
Clin
N Am)
Slide15Posterior Tibialis
Difficulty with ability to do a heel rise. Also check as the foot goes into plantar flexion, does the
calcaneus
invert (if functioning correctly) or does the heel stay in
valgus
Has been broken down into a 3 stages, with the more typical presentation in running at the first stage, synovial inflammation within the sheath and/or
paratendon
.
(Pelletier-
Galarneau
M, et al. 2015 Am J
Nucl
Med Mol Imaging)
Slide16Posterior Tibialis Treatment
Acute: activity modification, potentially with a walking boot, and relative rest. Ice, NSAID’s or iontophoresis.Strengthening of PF’s Foot orthosis/tapingInjections?
Slide17Plantar Fascitis
Has been reported to be present in about 8% of runners with musculoskeletal problems and has a lifetime
prevalence
of 10%
(Kindred J, et al 2011 Current Sports Medicine Reports)
No clear etiology, but is thought to be mechanical (
Pes
planus
, excessive
pronation
, decreased DF, increased daily WB, and obesity.
Bone spur??
Slide18Plantar Fascitis
Windlass mechanism – with toe DF during heel off pulls the plantar fascia tight, locking the midfoot and attempting to prevent longitudinal arch collapse. Conservative treatment can include stretching, taping, orthotics, strengthening, modalities, night splints (Tenforde A, et al 2016 Phys Med Rehabil Clin N Am)
Slide19Ankle Sprains
Studies have shown that 1/3 of female and ¼ of male high school age runners have a history of an ankle sprain (Tenforde AS, et al)Lateral ankle sprains are the most commonEvaluate the ligamentous structures, check for syndesmotic injury (not as common)
Slide20Ankle Sprains
PRICEReduction of edema and establishing pain free ROMPostural and balance exercisesStrengthening the intrinsic and extrinsic muscles of the foot and ankle as well as proximally.
Slide21Bone Stress Injuries
Metatarsal stress fractures are the second most common stress fracture in athletes and the most common in the foot.
Muscular fatigue with running increases stress to the metatarsals, with the 2
nd
, 3
rd
, and 4
th
metatarsals account for 90% of the fractures
2
nd
is most vulnerable secondary to it’s anatomic rigidity.
(
Bischof
J, et al, 2010 Gait Posture)
(Kennedy JG, et all, 2005 Current Opinion in Pediatrics)
Slide22Stress Fractures
Risk Factors:
Previous bone stress injury
Load applied to the bone – Training and biomechanical issues (loading rate, impact force, braking impulse).
Factors influencing ability of bone to resist load (physical activity history, energy availability, calcium and Vitamin D status.
Slide23Stress Fractures
Metatarsal stress fractures usually occur from a change in running frequency, duration or intensity.
Usually pain is without a specific MOI and early on it is relieved with rest. If running continues, the pain tends to become more consistent throughout ADL’s.
Look for focal tenderness, swelling.
To screen for tendonitis
vs
stress fracture – resist toe extension as this should not be a positive test with a stress fracture.
Slide24Stress Fracture
Risk factors:
Previous bone stress injury
Bone stress – load applied to it. Training errors or biomechanical – loading rate, impact force, and braking impulse.
Factors influencing the ability of bone to resist load (Bone mass and cross sectional area)
Kinematic Predictors: Center of mass to heel distance at initial contact. Angle of inclination at initial contact. Foot inclination angle and step width.
Slide25Biomechanics
Slide26Stress Fractures
Clinical decisions to make in the return to running
Location and severity of the injury
Impact free duration
Any previous running related injuries
Vitamin/Nutrition deficiencies
Running Experience
Slide273 Phases of Return to Running
Phase one: NWB to beginning weight supported Phase two: Impact preparation for controlling GRF and deceleration drillsPhase three: Impact tolerance, reduction of GRF’s, bounding drills.
Slide28Return to Running
Slide29Nerve Injuries
Neuromas (most commonly between the third and fourth metatarsals). Affects women 10x more than males – most likely because of a more narrow toe box.Presents with pain, tingling numbness to web space.Trials of shoe wear modification or inserts to reduce pressure at MET headsTarsal Tunnel Syndrome – injury to the posterior tibial nerve as it goes below the flexor retinaculum on the medial side of the ankle. Does not like to be compressed and often times seen in runners who run barefoot or in minimalist shoes. (Ferkel E, et al 2015 Clin Sports Med)
Slide30Tarsal Tunnel
Slide31Tarsal Tunnel
Tarsal Tunnel contains: posterior
tibial
nerve, posterior
tibialis
, flexor
hallucis
longus
, flexor
digitorum
longus
, posterior
tibial
artery/vein.
Symptoms: burning, tingling and shooting pain along the heel and medial aspect of ankle. Symptoms increase with standing, walking, running.
Ankle instability can be a contributing factor.
Slide32Running Shoes
Slide33Shoes
Slide34Running Mechanics
Slide35Conclusion
Thank You!
Slide36References
Kindred J,
Trubey
C, Simons S. Foot injuries in runners. Current Sports Medicine Reports. 2011; 10(5):249-254.
Tenforde
A, Yin A, Hunt K. Foot and ankle injuries in runners. Phys Med
Rehabil
Clin
N Am. 2016; 27:121-137.
Rabin A,
Kozol
Z,
Finestone
A. Limited ankle
dorsiflexion
increases the risk for mid portion
achilles
tendinopathy
in infantry recruits: a prospective cohort study. J Foot Ankle Research. 2014; 7:48.
Azevedo
L, Lambert M, Vaughn C, O’Connor C,
Schwellnus
M. Biomechanical variables associated with Achilles
tendinopathy
in runners. Br J Sports Med. 2009;43:288-292.
Creaby
M, Honeywell C,
Franettovich
M,
Schache
A,
Crossley
K. Hip biomechanics are altered in male runners with
achilles
tendinopathy
. Med
Sci
Sport and Exercise. 2016;549-554.
Kim S, Yu J. Changes of gait parameters and lower limb dynamics in recreational runners with
achilles
tendinopathy
. J Sports Science and Medicine. 2015; 14:284-289.
Agresta
C, Brown A. Gait retraining for injured and healthy runners using augmented feedback: a systematic literature review. JOSPT. 2015; 45(8):576-585.
Smith M, Honeywell C,
Wyndow
N,
Crossley
K,
Creaby
M.
Neuromotor
control of
gluteal
muscles in runners with
achilles
tendinopathy
. Med and Science in Sports and Exercise. 2014; 594-599.
Yu J. Comparison of lower limb muscle activity during eccentric and concentric exercises in runners with
achilles
tendinopathy
. J Phys
Ther
Sci. 2014; 26:1351-1353.
Matias
A,
Taddei
U, Duarte M, Sacco I. Protocol for evaluating the effects of a therapeutic foot exercise program on injury incidence, foot functionality and biomechanics in long-distance runners: a randomized controlled trial. BMC Musculoskeletal Disorders. 2016;17:160.
Warden S, Davis I,
Fredericson
M. Management and prevention of bone stress injuries in long distance runners. JOSPT. 2014;44(10):749-765.
Slide37References
Ferkel
E, Davis W, Ellington J. Entrapment neuropathies of the foot and ankle.
Clin
Sports Med. 2015; 34:791-801.
Nielson R,
Buist
I,
Parner
E,
Nohr
E, Sorenson H, Rasmussen. Foot
pronation
is not associated with increased injury risk in novice runners wearing a neutral shoe: a 1 year prospective cohort study. Br J Sports Med. 2014; 48:440-447.
Kennedy J, Knowles B, Dolan M,
Bohne
W. Foot and ankle injuries in the adolescent runner. Current Opinion in Pediatrics. 2005; 17:34-42.
Worp
M,
Wijer
A,
Staal
J,
Nijhuis
-van
der
Sanden M. Reproducibility of and sex differences in common
orthopaedic
ankle and foot tests in runners. BMC Musculoskeletal Disorders. 2014; 15:171.
Barnes R, Smith P. The role of footwear in minimizing lower limb injury. J Sports Sci. 1994; 12:341-353.
Bishop M, et al. Athletic footwear, leg stiffness, and running kinematics. J
Athl
Train. 2006; 41:387-392.
Kurz
M,
Stergiou
N. The spanning set indicates that variability during the stance period of running is affected by footwear. Gait Posture. 2003; 17:132-135.