
1 Contact haematologist on call document DOAC taken and last time drug ingested calculate creatinine clearance Cockcroft Gault FBC and check INRAPTTthrombin time Dabigatran Rivaroxaban ID: 1036452
Download Presentation The PPT/PDF document "Direct oral anticoagulant (DOAC) haemorr..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





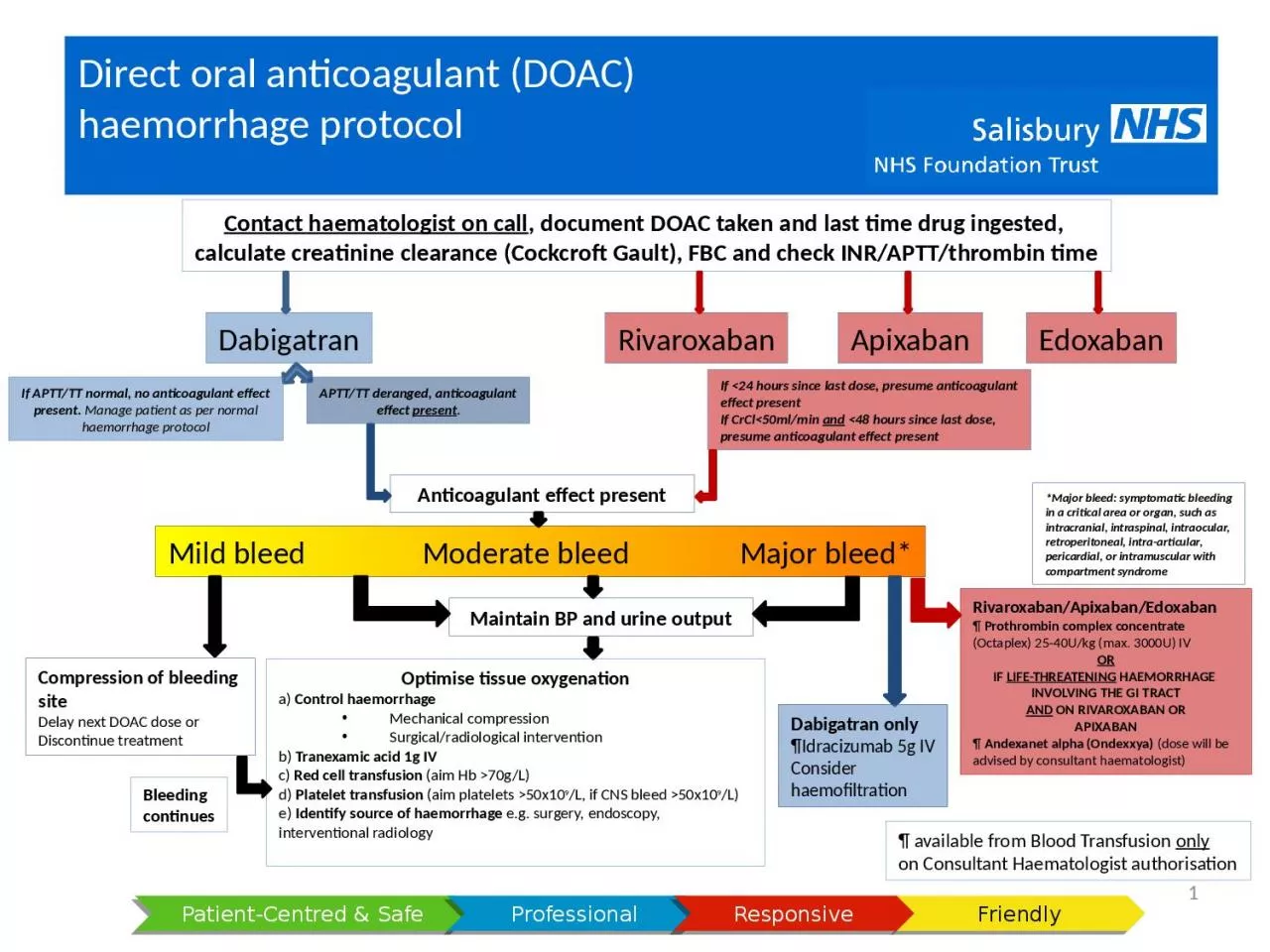
1. Direct oral anticoagulant (DOAC) haemorrhage protocol1Contact haematologist on call, document DOAC taken and last time drug ingested, calculate creatinine clearance (Cockcroft Gault), FBC and check INR/APTT/thrombin timeDabigatranRivaroxabanApixabanEdoxabanIf <24 hours since last dose, presume anticoagulanteffect presentIf CrCl<50ml/min and <48 hours since last dose,presume anticoagulant effect presentAnticoagulant effect presentMild bleed Moderate bleed Major bleed*Maintain BP and urine output*Major bleed: symptomatic bleedingin a critical area or organ, such asintracranial, intraspinal, intraocular,retroperitoneal, intra-articular,pericardial, or intramuscular withcompartment syndromeCompression of bleeding siteDelay next DOAC dose orDiscontinue treatmentOptimise tissue oxygenationa) Control haemorrhageMechanical compressionSurgical/radiological interventionb) Tranexamic acid 1g IVc) Red cell transfusion (aim Hb >70g/L)d) Platelet transfusion (aim platelets >50x109/L, if CNS bleed >50x109/L)e) Identify source of haemorrhage e.g. surgery, endoscopy, interventional radiology BleedingcontinuesDabigatran only¶Idracizumab 5g IVConsiderhaemofiltration Rivaroxaban/Apixaban/Edoxaban¶ Prothrombin complex concentrate(Octaplex) 25-40U/kg (max. 3000U) IVORIF LIFE-THREATENING HAEMORRHAGE INVOLVING THE GI TRACTAND ON RIVAROXABAN ORAPIXABAN¶ Andexanet alpha (Ondexxya) (dose will beadvised by consultant haematologist)¶ available from Blood Transfusion onlyon Consultant Haematologist authorisationAPTT/TT deranged, anticoagulanteffect present.If APTT/TT normal, no anticoagulant effectpresent. Manage patient as per normalhaemorrhage protocol