
JOHN Christein Grandview Cancer Center Program Overview Demographics Grandview Cancer Center Alabama Oncology Pancreatic cancer Care Program Definitions Operative strategies Grandview Cancer Center ID: 908951
Download Presentation The PPT/PDF document "Resection Extent for Pancreatic cancer" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

Slide1
Resection Extent for Pancreatic cancer
JOHN ChristeinGrandview Cancer Center
Slide2Program Overview
DemographicsGrandview Cancer Center/ Alabama Oncology Pancreatic cancer Care ProgramDefinitions
Operative strategies
Slide3Grandview Cancer CenterComprehensive Pancreatic cancer Care
Our team3 medical oncologists2 surgeons
Nurse4 care coordinators New Pancreatic cancer cases2019 200 new cases2020 220 new casesPancreatic operations2019 -2020 320 pancreatic operations (139 whipples
)
Slide4Grandview Cancer CenterComprehensive Pancreatic cancer Care
An example of a patient we would see every weekClinic on TuesdayMeet with medical oncologist and CoordinatorMeet with Surgeon
Meet with radiation oncology if neededStaging scans and labs if neededPort on FridayChemo starts on Friday
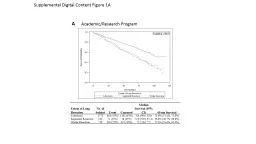
Slide5Prognostic factors associated with resectable adenocarcinoma of the head of the
pancreasRush University
75 patients48% adjuvant chemoZero neoadjuvant chemo17% 5 year survival
American Surgeon July 1999
My first publication
Slide61999 Pancreatic cancer Stats
28,600 new cases28,600 deaths
2021 PANCREATIC CANCER STATS60,430 new cases
48,220 deaths
Slide7Pancreatic Cancer: Scope of the Problem
2021 - 60,430 new cases of pancreatic cancer in us, 48,220 deaths
[1]Stage for stage, the lowest survival rate of any major cancer Only 20% operable at presentation
Metastatic disease or unresectable
By 2030,
pancreatic cancer
will be the
2nd
leading cause of cancer-related
Death
in the
US (after
lung cancer)
[2]
1. Siegel.
CA Cancer J Clin. 2020;70:7.
2. Rahib. Cancer Res. 2014;74:2913.
Slide82021 Pancreatic cancer staging
Slide92021 Pancreatic cancer staging
N0
Slide102021 Pancreatic cancer staging
T3
N0
Slide112021 pancreatic cancer staging
T1-3
N1
Slide122021 pancreatic cancer staging
N2 or
T4
Slide13Problems with pancreatic cancer staging
N2 definition just introducedNo radiology definition of Nodal positive diseaseNo post-neoadjuvant definitionsReally can only determine after resectionDoesn’t really help in determining role of neoadjuvant
therapyNccn guidelines don’t really utilize staging in recommendations
Slide142021 nccn Guidelines pancreatic cancer
Locally advanced disease or borderline resectable diseaseNeoadjuvant chemotherapyResectable diseaseConsider Neoadjuvant chemotherapy
New Guideline – First time to almost recommend neoadjuvant for all
Slide15Ideal staging system
Resectable – based on definitionsConsider neoadjuvant chemotherapyLocally advanced – based on definitionsNeoadjuvant chemotherapy +/- SBRTUnresectable – based on definitions
Neoadjuvant chemotherapy + sbrt/definitive rtMetastaticPalliative chemotherapy/immunotherapy
Slide16Slide17Slide18Slide19Slide20Slide21Slide22Slide23Slide24Slide25Slide26Slide27Slide28A root-cause analysis of mortality following major
pancreatectomyPancreatic Surgery Mortality Study Group
36 surgeons15 institutions, 4 countries12,000 patients (500 were mine)
5 intraop deaths
1.9% 90 day mortality
Journal of Gastrointestinal Surgery January 2012
Slide29whipple
Slide30Distal pancreatectomy/splenectomy
Slide31Multimodality therapy for pancreatic cancer in the U.S. : utilization, outcomes, and the effect of hospital
volumeNorthwestern University
National Cancer Database30,000 patientsLess than 51% received adjuvant chemo
Cancer Sept 2007
Slide32Neoadjuvant Therapy for Resectable Pancreatic Cancer: A New Standard of Care. Pooled Data from Three Randomized Controlled
Trials
Swiss, Germany, Italy3 Randomized Controlled Trials130 patients – operation vs neoadjuvant chemo then operationLonger disease free survival
Annals of Surgery July 2021
Slide33Perception versus reality: A National Cohort Analysis of the surgery-first approach for resectable pancreatic
cancer
Mayo12,000 patientsLonger survival after neoadjuvant (30 vs 20 mos)
Cancer Med July 2021
Slide34Often vein resection during whipple
Slide35Our approach for pancreatic head cancer
Neoadjuvant chemotherapyIf vein becomes 90 degrees then whipple with vein resectionIf vein stays close to 180 degrees then sbrt then whipple with vein resection
Slide36Prognostic Impact of Resection Margin Status in Distal Pancreatectomy for Ductal
AdenocarcinomaNorway
125 patientsConclusions:
Pathology examination is a key determinant of resection margin status following DP for PDAC. A high R1 rate is to be expected when pathology examination is meticulous and standardized. Involvement of the anterior pancreatic surface affects prognosis.
Annals of Surgical Oncology July 2021
Slide37Distal pancreatectomy for resectable adenocarcinoma of the body and tail of the
pancreasMayo
93 patientsEn bloc extended resections for T3
colon, kidney, stomach, duodenum, adrenal
Survival similar
to standard resection for T1, T2
Journal of Gastrointestinal Surgery 2005
Slide38Long-Term Results of Resection of Adenocarcinoma of the Body and Tail of the Pancreas Using Radical Antegrade
Modular Pancreatosplenectomy Procedure
Dr StrasbergWashington University, St Louis
81% R0 including tangential margins
30% 5 yr survival (before neoadjuvant era)
Journal of the American College of Surgeons 2012
2007
2003
Slide39Wider resections
Slide40Our approach to pancreatic body/tail cancer
Neoadjuvant chemotherapyIf portal vein involved then ramps with vein resectionIf adjacent organ involvement then ramps with en bloc resectionIf celiac or sma involvement then sbrt then ramps and skeletonize vessels
Slide41Comprehensive Pancreatic Cancer Care
Scheduled within a week of requestMultidisciplinary first appointmentTreatment to start within 7 daysPossible to start in 3 days
John.christein@alabamaoncology.com
205-410-6951