

Cleveland Clinic Florida Breast Surgeon September 25 2018 Breast Cancer Highly prevalent disease Limited to female sex in all but lt 1 of cases in USA SEER Cancer Stat Facts Female Breast Cancer ID: 913403
Download Presentation The PPT/PDF document "Breast Cancer in Men Margaret Thompson M..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.







Slide1
Breast Cancer in Men
Margaret Thompson MD
Cleveland Clinic Florida
Breast Surgeon
September 25, 2018
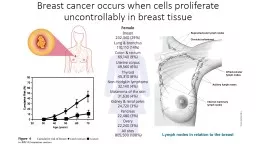
Slide2Breast Cancer
Highly prevalent disease
Limited to female sex in all but < 1% of cases in USA
Slide3SEER
Cancer
Stat Facts: Female Breast Cancer
Slide4Slide5Slide6Slide7Slide8Detection and Presentation
No studies to address the role of early detection in men
Screening mammogram has limited role in men than women
Due to anatomic & pathologic differences
≈
85% of male breast cancers are evident on P/E
Predominantly central
subareola
location
Limited volume of breast tissue
Slide9Detection and Presentation
For most healthy patients
Periodic self-examination
Annual physical examination
For cancers detected in this way, most present with self-detected mass
Other symptoms
Nipple discharge
Ulceration
Bleeding
Skin inversion
Swelling
Breast pain
Compared with BC in women, nipple symptoms more common (48%)
R/T proximity of male BC to the nipple-areola complex (NAC)
Slide10Detection and Presentation
Average duration of symptoms = 4-18 months
Patients with family history of breast cancer
Significantly shorter duration of symptoms = 1 month
Diagnosis delay strongly r/t lack of awareness of BC in men
Historical series shows a more advanced stage at presentation
With an associated delay in diagnosis
More contemporary series show more smaller tumor diameter at presentation
Suggesting ↑ public & professional awareness
Slide11Differential Diagnosis
Gynecomastia
Limited to men
Hypertrophy of breast
Bilateral / unilateral
Tenderness
P/E = diffusely enlarged breast, firm /tender, overlying skin normal; nipple deformities / discharge unusual
Epidermal inclusion cyst
Lipoma
Subareola
abscess
Fat necrosis
C
hronic inflammation
H
ematomas
Slide12Differential Diagnosis
Metastatic disease to the breast
Most common – metastatic prostate cancer
Share similar demographic features
Older patient in whom prevalence of gynecomastia is ↑
In patient with known history of prostate cancer, 3 diagnostic possibilities emerge
Gynecomastia
Metastatic prostate cancer
Breast cancer
Metastatic prostate cancer & 1
°
breast cancer have been ID in same breast following initiation of hormonal therapy for metastatic prostate cancer
Other
1
° tumors reported
Colon cancer, osteosarcoma, Ewing's sarcoma, lung cancer, lymphoma, laryngeal ca,
Malignant melanoma, Bowens ds
Slide13Risk Factors
Age
Risk ↑ as
men
age
Average age
72 years old when
diagnosed
Family history of BC
BC risk ↑
if
other blood relatives have had BC
1 of
5 men with
BC have
a close relative, male or female, with the disease
Slide14Epidemiology, Risk Factors & Genetics
Genetic predispositions play important role in
pts
with
fam
hx
of male BC or both male & female BC
Initial reports implicated BRCA2, to account for as many as 14% of male
pts
with inherited BC
More recent reports BRCA2 mutations account for 40% of all male BC in Iceland
BRCA1 mutations, although uncommon, may also account for familial cases of male BC
Slide15Genetics
+ family history of BC in 1
°
relative is ID in 15% of male BC
pts
All male BC patients should consider genetic counselor consultation
Especially if they have premenopausal 1
°
relatives with
hx
of BC
Or multiple family members with BC or ovarian cancer
Men with BRCA2 mutation carry a 6.3% lifetime risk of BC
Intervention
Heightened surveillance
Chemoprevention
Prophylactic mastectomy
Slide16Slide17Slide18Slide19Tamoxifen ↓ BC risk in women (STAR Trial)Used in treatment of male BC with good safety profile
Prevents only ER+ tumors
Predominant receptor profile in male BC
Chemoprevention
Slide20Risk Factors
Cowden’s syndrome
Autosomal Dominant
Multiple
hemartoma
syndrome
Assoc
w/
germline
mutation
PTEN
tumor-suppressor gene
3 reported cases of Cowden’s syndrome have occurred in men
2 led to lethal BC developing while patients were in their early 40s
Multiple
lipomas
of various sizes on the torso (a), limbs (b) and on the left thumb basal joint right (c)
Slide21Risk Factors
Klinefelter’s
syndrome
XXY karyotype hormonal condition
Hypogonadism
Gynecomastia
Aspermatogenesis
Obesity
Genetic predisposition of 20-
to 50-fold
↑
BC risk
Slide22Risk Factors
Alcohol
↑ alcoholic intake ↑risk of male BC
Possible d/t effects on liver
Liver disease
Liver plays important role in balancing sex hormones levels
In severe liver disease (cirrhosis)
Hormone levels are uneven
Causing < levels of androgens & > estrogen levels
Men with liver disease have a > chance of developing
gynecomastia
They have > risk of developing breast cancer.
Slide23Risk Factors
Radiation exposure
Men who have had previous chest radiation (mantle radiation for lymphoma) has
an
↑risk
of developing breast cancer
Estrogen
treatment
Once
used in hormonal therapy for
prostate cancer treatment
This
treatment may
slightly ↑ BC risk
Concern
that transgender/transsexual individuals who take high doses of estrogens as part of sex reassignment could also have
> BC risk
No studies
of
BC risk
in transgendered individuals, so it isn’t clear what their breast cancer risk
is
Slide24Risk Factors
Obesity
Studies show
women’s BC risk
↑
with postmenopausal
obesity
Obesity also risk
factor for male breast cancer
Fat
cells convert
androgens
into
estrogens
Obese
men have higher levels of estrogens
Testicular Conditions
Undescended testicle
Adult mumps
Uni
/ bilateral orchiectomy
Slide25Pathology
Similar diversity as in women
Lobular male breast cancers previously thought non existence
Because of normally absent terminal lobular unit
Several cases ID for both in situ & invasive lobular cancer
Every histologic entity described in women has occurred in men
In men, mostly ductal type
Most common subtype is invasive papillary cancer
Metastatic patterns similar to women
Lung, adrenal, & bone accounts for most
Slide26Pathology
DCIS distribution in men differs
DCIS 40% mammogram detected cancers in women <50
yo
<5% of all male BC are DCIS
Contralateral BC <2% of men
Inflammatory BC uncommon, but have been described
Superficial dermal
lymphatics
are invaded, leading to edema & vascular congestion
Peau
d’orange
/ hyperemia
Paget’s Disease
Nipple ulceration, bleeding, crust formation w/associated mass
Treatment is analogous to that of invasive ductal cancer
Most male BC are ER+ (87%)
ER+ in men remain constant / independent of age
In contrast, ER+ ↑ with age for women
Slide27Staging
AJCC staging scheme applies identical criteria to both men & women
AJCC
system, effective January 2018, has both clinical &
pathologic staging
systems
Clinical stage
Results
of
physical
exam, biopsy,
&
imaging testsUsed
to help plan
treatment
Pathologic
stage
(also called
surgical
stage
)
Determined
by examining tissue removed during
surgery
T
, N,
&
M
categories
ER
, PR, Her2 status
Grade
of
cancer
Slide28Staging
Comparative review of both 1999-2005, BC in men
Present with larger T
Higher frequency of LN+ (37% vs 22%)
Large median size of nodal
mets
(10 vs 3mm)
Chest wall fixation more common in men
But does not affect prognosis as it does in women
Normal anatomic proximity of breast to skin / muscle accounts for frequency of this finding
Slide29Diagnostic Evaluation
P/e reveals palpable mass
FNA can give diagnosis
Properly obtained specimenAdequate material
Experience
cytopathologist
CNB will provide more information
+/- mammogram for
ipsilateral
or contralateral breast
Subareolar
breast mass with ↑ density / architectural distortion
Calcifications < common, coarser than seen in women
+/- ultrasound
Image-guided core needle biopsy
Slide30Diagnostic Evaluation
Nipple discharge presentation
Collect sample for cytology
DCIS has been described on male nipple ductal secretions
+/-
Ductography
Metastatic work up
For stage II or more advanced disease
Bone scan, LFTs, CT chest, abdomen, pelvis
Identification of
mets
should alter treatment from local to systemic therapy
Slide31Case Presentation
82
yo
Caucasian male of Ashkenazi Jewish descent who presents
with
LEFT
palpable mass with aching pain in left side of his
chest x few months.
He
also says that his left nipple has become
inverted
x few
wks
Otherwise
he denies unexplained weight loss, back/bone pain, abdominal pain, memory/
neuro
deficits.
Does admit to persistent cough.
RISK FACTORS:
No liver disease, hormone
tx
, prostate issues.
Family history of breast cancer: Yes, Sister, lumpectomy
79
for breast cancer
Family history of other cancers: Yes, Father, liver 85.
Smoker: Yes, Quit 40 years ago. Smoked 1 pack per day 18-28 and 32-35.
Of Ashkenazi Jewish descent
Slide32P/e LEFT central 2 cm breast mass with nipple inversion, no skin changes, no axillary LAD
Mammogram
1.7
cm x 1.7 cm
mass
spiculated
margin
linear calcifications
correlates
as
palpated
nipple retraction
assoc
w/mass
HIGHLY
SUGGESTIVE OF
MALIGNANCY
Ultrasound recommended
Slide33ultrasound
0.5
cm x 1.3 cm x 1.6 cm irregular mass
left
breast central to
nipple
anterior depth is highly suggestive of malignancy. An
ultrasound
guided biopsy is recommended
.
The 0.9 cm lymph node with focal cortex thickening
left
axilla is
suspicious of malignancy. An ultrasound guided biopsy is recommended.
Slide34LEFT USG CNB & CNB of axillary LN
Slide35Post biopsy clip
Slide36Ultrasound Guided CNB
LEFT BREAST, RETROAREOLAR, COIL CLIP, ULTRASOUND-GUIDED BIOPSY:
-
INFILTRATING CARCINOMA, DUCTAL TYPE, NOTTINGHAM SCORE 3+2+1=6/9.
- THE TUMOR MAXIMUM LINEAR DIMENSION IS APPROXIMATELY 9 MM.
- THE INFILTRATING CARCINOMA IS ASSOCIATED WITH
CALCIFICATIONS
LEFT
AXILLARY LYMPH NODE, CORE BIOPSY:
- FRAGMENTS OF BENIGN LYMPH NODE.
ESTROGEN
RECEPTOR
100
% nuclear staining with strong intensity
PROGESTERONE
RECEPTOR
100
% nuclear staining with strong intensity
HER2 EQUIVOCAL
(2+)
FISH
will be performed and results reported in an addendum.
FISH Analysis
HER2 Breast - LEFT BREAST
Results: Negative
Slide37PET scan
FDG
avid soft tissue density nodule
retroareolar
left breast in
keeping
with known neoplasm.
No
PET evidence of FDG avid
adenopathy
or
distant
metastatic disease
Slide38Case Presentation Genetic testing negative
LEFT simple mastectomy & LEFT SLNB
1.7 cm invasive ductal cancer, grade II
No LVI
0/3 negative SLN
Referred to medical oncology
Oncotype
pending
Slide39Surgical Treatment
Major anatomic difference b/w men & women is size of breast & absent breast mound
Leads to differences in local therapy in men
Proportional size of tumor to breast volume is important criteria for selecting of breast conservation
Other major anatomic difference is spatial relationship between the nipple-areola complex (NAC) & breast tissue
Closely related in men, it is often impractical to preserve the NAC
Given the large amount of breast tissue excised & loss of NAC, breast conserving approach is not indicated for most male BC patients
Slide40Surgical Treatment
Psychosocial impact of mastectomy has not been formally addressed in male cohorts
Safe assumption that the breast has a greater value for women in terms of functionality, sexuality, body image, & symmetry
Local therapy for most male BC is mastectomy
NCDB of ACS men (75%) > treated with mastectomy than were women (59%)
LABC should be evaluated for NACT
Slide41Surgical Treatment
Simple mastectomy – removal of breast only
Modified radical mastectomy – removal of breast & axillary LNs
Radical mastectomy for those with
pectoralis
muscle involvement
Breast reconstruction seldom considered in men
Latissimus
flap or TRAM
Axillary staging
Sentinel Lymph Node Biopsy
Axillary Lymph node dissection
Slide42Surgical Treatment
Post
mastectomy closure of the skin defect by
pedicled
latissimus
dorsi
myocutaneous
flap
Slide43Radiation Therapy
Proximity b/w most male BC & skin & chest wall
Extension to or invasion > common than in women
Chest wall involvement in male patients does not portend a different prognosis than that found in patients without involvement
For most, these findings should lead to consideration of radiotherapy
Although no randomized clinical data available
Radiotherapy does ↓ risk LR in men
Extensive or
extracapsular
nodal involvement predictors of regional failure in women
Also apply as criteria for post op XRT in men
NCDB: men more likely to receive
postmastectomy
XRT than women
29% vs 11%, p=0.001
Slide44Systemic Treatment
Stage, age at diagnosis, hormone receptor status
Variables that affect adjuvant systemic therapy
Men have > advanced stage on presentation, ↑ risk of systemic relapse & potential benefits of adjuvant treatment
Also present at later age & therefore have more frequent comorbidities that may limit choices of systemic therapy
Most male BC are ER+, allowing for use of hormone therapy
Which leads to an improvement in survival
Slide45Systemic Therapy
Chemotherapy
L
imited
frequency of use in men (26%) compared to women (40%), p=0.001
But has a role in more aggressive ds providing patient has adequate performance status
Retrospective review 156 male BC at MD Anderson
51 of 135 with
nonmets
BC received either adjuvant chemo, hormonal
tx
, or both
Men with LN+, adjuvant chemo
assoc
w/ lower risk of death (HR 0.78), not stat sig.
OS was
significantly better for men who received adjuvant hormonal therapy (HR 0.45, P=0.01)
Slide46The 21-Gene Recurrence Score Assay (Oncotype DX™) in Estrogen Receptor-Positive Male Breast Cancer: Experience in an Israeli Cohort
Grenader
et al
Oncology 2014;87:1-6
Assess
Recurrence Score
in
Israeli male breast cancer (MBC)
patients
N = 65
RS
assay (
Oncotype
DX™)
performed
on paraffin-embedded tumor samples at Genomic Health
laboratories
Results
Mean
age
65.1
yrs
(38-88
yrs
)
Low-risk
(RS <18), intermediate-risk (RS 18-30)
& high-risk
(RS ≥31) scores were noted in 29 patients (44.6%), 27 patients (41.5%)
&
9 patients (13.9%),
respectively
Distribution
of RS in male patients
similar
to
distribution
in 2,455 female patients from Israel referred during the same time
period
Conclusion
Data
suggest
the
distribution of
Oncotype
DX RS in
ER +
MBC patients is similar
to
female breast cancer
patients
Slide47Slide48