PPT-Lecture #9 First semester
Author : candy | Published Date : 2024-01-03
Cardiovascular D isorders I Hypertension Al Mustaqbal University College College of Nursing 2 nd Class Adult Nursing by lecturers DrFakhria Jaber Definition
Presentation Embed Code
Download Presentation
Download Presentation The PPT/PDF document "Lecture #9 First semester" is the property of its rightful owner. Permission is granted to download and print the materials on this website for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.
Lecture #9 First semester: Transcript
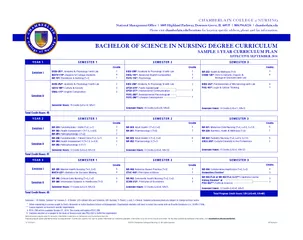
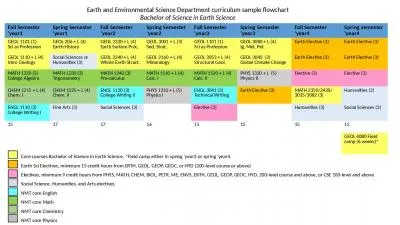
Cardiovascular D isorders I Hypertension Al Mustaqbal University College College of Nursing 2 nd Class Adult Nursing by lecturers DrFakhria Jaber Definition. Writing FSAW 3 Fundamental Studies Math FSMA 3 GVPT170 DSHS 3 Abstract Thinking Skills st of 3 3 Semester 2 16 credits Taken Semester CompletedAnticipated JOUR201 3 Natural Lab Science DSNL 4 COMM107200 FSOC 3 Humanities DSHU 3 A nyuedu Chapter 3 Variance Reduction 1 Introduction Variance reduction is the search for alternative and more accurate estimators of a given quantity The possibility of variance reduction is what separates Monte Carlo from direct simulation Simple var August 25 Ending date June 4 Staff Starting date August 15 Ending date June 5 Student Holidays Labor DaySeptember 1 Thanksgiving November 2428 Winter Break Dec 22 Jan 5 Martin Luther King January 19 Presidents DayFebruary 16 Spring Break March 16 5 L05 NR281 Pathophysiology I T2 Credits NR324 Adult Health I T3 C2 NR291 Pharmacology I T2 Credits NR321 MaternalChild Nursing T3 L05 C15 NR228 Nutrition Heath Wellness T2 Credits Session II NR226 Fundamentals 57526 Patient Care T2 C1 NR304 Health Paul Sava. Department of Geophysics. Colorado School of Mines. Geophysics:. an . applied and interdisciplinary science. CSM Geophysics program. Department of Geophysics. Colorado School of Mines. College of Earth Resource Sciences and Engineering. Business English 3. . 2nd year. Graduate programme. Academic year 2016/17. Winter semester. Lecturer: . MSc Sanda Katavić-Čaušić. “Education is our passport to the future,. for tomorrow belongs to the people. Arya, . Vipin. , Lilian:. More slides will follow. Lecture 5 - Introduction. 3 Strategic Goals of this course. 4 Tactical Goals of this course. What is Computation – Philosophy – 2 forms of knowledge. 2016. Dr. Phillip Bogle, Ph.D.. Program Coordinator. . RPED . 251 . Meeting Outline. Course Textbook Concerns. Plans for new RPED . 250/251 . Examination Guidelines. Scheduling . Teaching Evaluations . November 8. th. , 2016. Semester in San Francisco 2012. 2. SSF Cohort 2012. Net Promoter Score . higher . than Apple iPhone at it’s peak. Q2 NPS = 74%. 2010 Apple iPhone NPS = 73. %. Students said…. CodeTitlePrereqTPECTSMATH201Linear Algebra216CEIT201Office Operations216PSY103Introduction to Psychology216University Elective 1 Table 16University Elective 2 Table 23Foreign Language Elective I Table CodeTitlePrereqTPECTSTLT104Turkish Language I Turkish Phonetics216TLT113Turkish Oral Communication Skills216PSY103Introductionto Psychology216University Elective 1 Table 16University Elective 2 Table Introduction to Physical Science. 4-credit conceptually-oriented course with some algebra and with integrated laboratory component.. The course focuses on physics concepts.. Serves primarily . Speech-language Pathology Majors . Programming and Data Structure. 1. Introduction to C. C is a general-purpose, structured programming language.. Resembles other high-level structured programming languages, such as Pascal and Fortran-77.. Semester ‘year1. Fall Semester ‘year2. Spring Semester ‘year2. Fall Semester ‘year3. Spring Semester ‘year3. Fall Semester ‘year4. Spring semester ‘year4. GEOL. 1101 (1). Sci as Profession.
Download Document
Here is the link to download the presentation.
"Lecture #9 First semester"The content belongs to its owner. You may download and print it for personal use, without modification, and keep all copyright notices. By downloading, you agree to these terms.
Related Documents