
Dr S Parthasarathy MD DA DNB MD Acu Dip Diabetes DCA Dip Software statistics PhD physiology IDRA FICA What is it It consists of a complex arrangement of ID: 1047577
Download Presentation The PPT/PDF document "Larynx – what to know !" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

1. Larynx – what to know ! Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diabetes, DCA, Dip. Software statistics- PhD ( physiology), IDRA, FICA
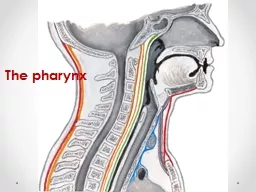
2. What is it ? It consists of a complex arrangement of muscles, cartilage, membranes and ligaments. It extends from C3 to C6 in the midlineHanging from the hyoid to trachea Some what higher in children( 2nd to fifth? cervical vertebrae) and femalesOrgan designed to coordinate deglutition respiration and phonation
3. What does it do ?? Breathing Preventing aspiration during deglutition Voice
4. Elevated epiglottis abutting the nasopharynx – more useful for aspiration prevention than phonation !!
5. Three levels of aspiration prevention
6. False vocal cords – inferior orientation - 30 mmHg--Develop a pressure to cough True vocal cords superior orientation – stops ingress of fluids – 140 mmHg – How difficult to ventilate in spasm !!
7. Male and female ??
8. Anatomy Anterior – superficial structure, is covered by the fascia platysma and skinPosterior –prevertebral , cervical vertebraeSuperior – pharynxInferior – becomes continuous with the trachea
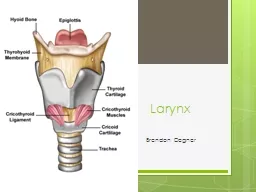
9. Structure Cartilages (nine) – three unpaired and six pairedLigaments Muscles
10. Total nine Epiglottis Thyroid Cricoid Corniculate Cuneiform Arytenoid
11. Epiglottis !!
12. Epiglottis (elastic) – ‘leaf’-shaped; the lower, narrower end is attached to the thyroid cartilage by the thyro-epiglottic ligament upper broader end is free to project superiorlymedian glossoepiglottic fold and pharynx as two lateral glossoepiglottic fold
13. In DeglutitionHyoid bone move upward and forwardEpiglottis bent posteriorly on laryngeal inletFood slips to the lateral surface Taste sensation Assist in phonation Gag reflexPrevent aspiration of food
14. Thyroid Two laminae FUSION MORE IN MALE Notch Superior and inferior cornua
15. Thyroid cartilage In females, the sides join at approximately 120 degrees In males at closer to 90 degrees. This smaller thyroid angle explains the greater laryngeal prominence in males (the “Adam's apple”), the longer vocal cords, and the lower pitched voice
16. Vocal cords at the lower border
17. Cricoid cartilage (hyaline) – ‘signet ring’-shaped and situated at the C6 level. It articulates on its lateral border with the thyroid cornua, and on its upper border with the arytenoid cartilages..
18. Cricoid cartilage. cricoid is derived from the Greek words krikos and eidos, meaning shaped like a ringOnly laryngeal cartilage- complete ringSmaller but thicker & stronger than thyroid
19.
20. The two light arytenoid cartilages are shaped like three-sided pyramids, and they lie in the posterior aspect of the larynx-posterior joint Crico arytenoid arthritis In rheumatoid and SLE The lateral extension of the arytenoid base is called the muscular process. Important intrinsic laryngeal muscles, lateral and posterior cricoarytenoids, originate here. The medial extension of the arytenoid base is called the vocal process.
21. Two sets of paired fibroelastic cartilages are embedded in each aryepiglottic fold.[ The cuneiform and corniculate cartilages reinforce and support the aryepiglottic folds and may help the arytenoids move
22.
23.
24. Only this opens Safe muscle of the larynx
25. It contracts in 14 seconds while posterior crico arytenoid in 44 seconds Mechanism to prevent aspiration
26. Elevation of larynx- thyrohyoid, mylohyoid Depression of larynx- sternothyroid, sternohyoid Abductors – Posterior cricoarytenoid Adductor - Lateral cricoarytenoid, interarytenoidRegulation of cord tension– Cricothyroid (Tensor)– Thyroarytenoid – (Relaxors)– Vocalis (fine adjustment)
27. Vascular supply Superior laryngeal artery - superior thyroid A Inferior laryngeal artery – inferior Thyroid A Crico thyrioid artery -superior thyroid A SLV – STV -- IJV ILV - Brachiocephaliv V
28. Nerve supply Epiglottis – glossopharyngeal nerve Above vocal cords – internal branch of superior laryngeal nerve Below vocal cords – recurrent laryngeal nerve Motor All muscles of the larynx are supplied by the recurrent laryngeal nerve except cricothyroid ( ext. branch – superior laryngeal nerve )
29. Right recurrent – Subclavian round Left – aortic arch rounding Lengthier
30. Voice Vibrations/ second of the vocal cord Pitch = L/TM Depends on:a. Length of VC.b. Mass of VC.c. Tension of VC.Men 90- 500 Hz Women – 150 – 1000
31. Vocal folds vibrate faster as they're pulled longer, thinner, and more taut and vibrate more slowly when they're shorter, thicker, and floppier.The cricothyroid muscle and thyroarytenoid muscle coordinate with each other to create different pitches.
32.
33.
34.
35. Thyro arytenoid causes relaxation When it is gone, tension – pitch goes up Cricothyroid – EXT – laryngeal nerve – tenses Problem to the nerve – relaxation – low pitch
36. Laryngeal paralysis can beUnilateral or Bilateral & may involve –1. Recurrent laryngeal nerve2. Superior laryngeal nerve3. Both (Combined / Complete)
37. The recurrent laryngeal nerve may be traumatized during surgery on the thyroid and parathyroid glands. Malignancy or benign processes of the neck, trauma, pressure from an ET or a laryngeal mask airway, and stretching the neck may also affect the nerve
38. 1.53.57.5
39.
40.
41.
42. Downloaded from net for closed academic purpose only
43. Bilateral recurrent N palsy All the intrinsic muscles of larynx are paralysed, vocal cords lie in median or paramedian position due to unopposed action of cricothyroid muscles.• Clinical features :- Dyspnoea stridor
44. This is normal !
45. Inspiration and expiration in BL RLN palsy
46. PARALYSIS OF SUPERIOR LARYNGEAL NERVEUnilateral Weak voice with decreased pitch- Anaesthesia of larynx on one side- Occassional aspiration.- Askew position of glottis - Ant. Comissure is rotated to healthy side.- Shortening of V.C. with loss of tension & V.C. appears wavy- Flapping of the paralysed vocal cord – V.C. sags down during inspiration & bulges up during expiration Bilateral Both V.C. paralysis- Anaesthesia of larynx- Cough- Chocking fits- Weak & husky voice
47. Bilateral incomplete RLN Addutors are intact !! On inspiration
48.
49. Summary Larynx – borders Cartilage Three levels of aspirationSensory supply Muscles and their action Safe muscle Various positions
50. What is the laryngeal activity which comes with class ? Yawning
51. Thank you