
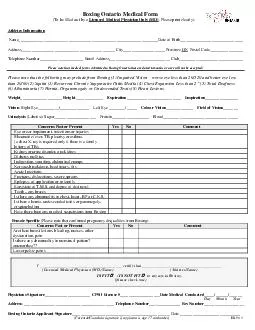
Patient First NameMIPatient Last NameDOBPhysician InformationPhysician First NamePhysician Last NameTitle DO MD etcName of PracticeMedical License NoStreet AddressCityZIP CodeDate of applicant146sla ID: 892137
Download Pdf The PPT/PDF document "Medical Verification FormThis form shall..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


![Has had the following childhood illnesses [please indicate date(s)]:Ch](https://thumbs.docslides.com/326891/has-had-the-following-childhood-illnesses-please-indicate-d.jpg)


1 Medical Verification FormThis form shall
Medical Verification FormThis form shall be completed by a physician licensed to diagnose your condition or disability and is able to provide the needed information that would help determineeligibility for ADA paratransit service. Incomplete forms will be returned. Patient First Name: MI: Patient Last Name: D.O.B. / / Physician Information Physician First Name: Physician Last Name: Title (DO, MD, etc.): Name of Practice: Medical License No.: Street Address: City: ZIP Code: Date of applicant’slastvisit: Medical diagnosis of disability/condition: Please describe PhysicianSignatureDate The original Medical Verification Form must be received within 30 days of the ADA Paratransit Application. Applications will only be considered completed