
CISICISI 2033995121 wwwculturalinsurancecom Cultural InsuranceServices International SCHEDULE OF BENEFITSBasic Plan Coverages Maximum limits ꔀper Accident or Sicknessper Accident or Sickness ID: 834762
Download Pdf The PPT/PDF document "River Plaza 9 West Broad Street Stamfo..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.








1 CISICISI River Plaza ¥ 9 West Broad Str
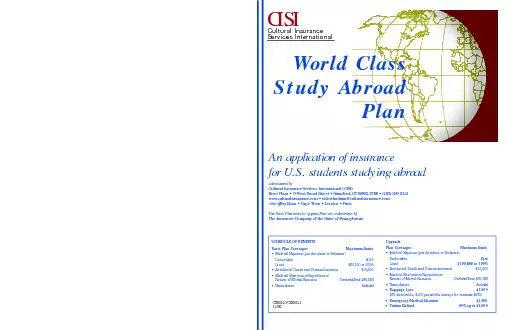
CISICISI River Plaza ¥ 9 West Broad Street ¥ Stamford, CT 06902-3788 203-399-5121 ¥ www.culturalinsurance.com Cultural InsuranceServices International SCHEDULE OF BENEFITSBasic Plan Coverages Maximum limits ꔀper Accident or Sicknessper Accident or SicknessDeductible$100 ꔀAccidental Death and Dismemberment$10,000ꔀMedical Evacuation/Repatriation/ Combined limit $50,000 ꔀTeam Assist Plan CoveragesMaximum limits ꔀper Accident or Sicknessper Accident or Sickness $100,000 at 100% ꔀMedical Evacuation/Repatriation/ Combined limit $50,000 Team Assist Baggage Loss$1,000 $50 deductible; $100 per arexcept for cameras $250except for cameras $250 Emergency Medical Reunion$1,500 uition Refund50% up to 11/06 An application of insurancefor U.S. students studying abroad ed by CISICISIRiver Plaza ¥9 West Broad Street ¥ Stamfor203203www.culturalinsurance.com ¥ cisiwebadmin@culturalinsurance.com other offices Bonn ¥ Cape Town ¥ London ¥ Paris The Basic Plan and the Plan are underwritten by The Insurance Company of the State of Pennsylvania World Class Study Abroad Covered Accident and Sickness Medical Expenses nly such expenses, incurred as the result of a Disablement, which arepecifically enumerated in the following list of charges, and which are notexcluded in the Exclusions section, shall be considered as Covered Expenses: ꔀCharges made by a Hospital for room and board, floor nursing andꔀCharges made for diagnosis, treatment and Surgery by a PhysicianꔀCharges made for an operating room.ꔀCharges made for Outpatient treatment.ꔀCharges made for the cost and administration of anesthetics.ꔀCharges for medication, x-ray services, laboratory tests and serv-ꔀCharges for inpatient physiotherapy, if recommended by aꔀDressings, drugs, and medicines that can only be obtained uponꔀCharges made for artificial limbs, eyes, larynx, and orthotic appli-ꔀLocal transportation to or from the nearest Hospital by licensedground ambulance only.ꔀNervous or Mental Disorders are payable a) up to $500 for outpa-ꔀChiropractic Care and Therapeutic Services shall be limited to a Eligibility Requirements Citizens of the U.S. who are enrolled as full-time students at U.S.institutions or on a recognized study abroad program and who aretemporarily engaged in international educational or cultural activi-ties outside their home country are eligible for coverage. For benefits listed in the Schedule of Benefits, this Insurance does not cover: ꔀPre-Existing conditions, defined as any Injury or Illness which meetscoverage under the Policy.ꔀSuicide or any attempt thereof, while sane or self destruction orꔀAny consequence, whether directly or indirectly, proximately orremotely occasioned by, contributed to by, or traceable to, or aris-ing in connection witha)war, invasion, act of foreign enemy hos-civil war; or b) mutiny, riot, strike, military or popular uprisingrection, rebellion, revolution, military or usurped power. ꔀThe refusal of a Physician or Hospital to make all medical reportsꔀCosmetic or plastic Surgery, except as the result of a co
2 vered acci-dent; for the purposes of the
vered acci-dent; for the purposes of the Policy, treatment of a deviated nasalꔀElective Surgery or Elective Treatment which can be postponeduntil the Insured Person returns to his/her Home County, where thebjective of the trip is to seek medical advice, treatment or Surgery.ꔀTreatment in connection with alcoholism and drug addiction, ordirected by a Physician for a condition which is covered hereunder.ꔀCongenital abnormalities and conditions arising out of or result-ꔀExpenses as a result or in connection with intentionally self-ꔀInjury sustained while taking part in mountaineering where ropesꔀDental care, except as the result of Injury to natural teeth causedꔀRoutine Dental Treatment.ꔀDrug, treatment or procedure that either promotes or preventstility or impotency, ster-dent pilot, operator or crew member, in or on, boarding or alight- Credit card enr203203 PARTICIPANT CONTACT INFORMATION: T__________________________ Female Male Date of birth ________/________/________ PROGRAM INFORMATION: U.S. institution where enrolled as student if applicableif applicable Institution sponsoring study abroad program if applicableif applicable Name of international institution you will attend____________________________________________________Host country _________________________Program start date ________/________/________Program end date ________/________/________ ENROLLMENT INFORMATION: I want my insurance to begin ________/________/________and continue for ________ months maximum 12 whole months onlymaximum 12 whole months only STUDYABROADPLAN ENROLLMENTFORM nroll on-line at www.culturalinsurance.com. 12/06 Basic Plan Rate (see Premium Rates section) $_________ x ________ mon whole months onlywhole months only = $__________ Total premiums= $__________ BeneficiaryÕs name________________________________________________ Relationship_____________________________ PAYMENT INFORMATION: Check/money order enclosed Visa MasterCard Please provide the following additional information for credit card payments:CardholderÕplease printplease printIhave read and understand the terms and conditions of the policy and authorize payment for the above enrollment. ocessing. All insurance materials are sent via standard U.S. Mail. Make checks payable (U.S.funds only) toCISIand mail with completed enrollment form to :CISI, River Plaza, 9 West Broad Street, Stamford, CT 06905-3788. Please contact CISIif you have any questions about this form or the policy. mm dd yymm dd yymm dd yymm dd yymm dd yymm yy Policy terms and conditions are briefly outlined in this document. A complete description is containedin the Plan of Insurance which you will receive after your enrollment. For office use only Participant ID# Premium Rates Basic Plan Monthly premium up to 25$3426-305141-6014661+261 Upgrade Plan MonthsAdditional premium 1-6$100*7-12200* Rates are valid until December 31, 2007. Full months only, plea
3 se. Covered Accident and Sickness Medica
se. Covered Accident and Sickness Medical Expenses nly such expenses, incurred as the result of a Disablement, which arepecifically enumerated in the following list of charges, and which are notexcluded in the Exclusions section, shall be considered as Covered Expenses: ꔀCharges made by a Hospital for room and board, floor nursing andꔀCharges made for diagnosis, treatment and Surgery by a PhysicianꔀCharges made for an operating room.ꔀCharges made for Outpatient treatment.ꔀCharges made for the cost and administration of anesthetics.ꔀCharges for medication, x-ray services, laboratory tests and serv-ꔀCharges for inpatient physiotherapy, if recommended by aꔀDressings, drugs, and medicines that can only be obtained uponꔀCharges made for artificial limbs, eyes, larynx, and orthotic appli-ꔀLocal transportation to or from the nearest Hospital by licensedground ambulance only.ꔀNervous or Mental Disorders are payable a) up to $500 for outpa-ꔀChiropractic Care and Therapeutic Services shall be limited to a Eligibility Requirements Citizens of the U.S. who are enrolled as full-time students at U.S.institutions or on a recognized study abroad program and who aretemporarily engaged in international educational or cultural activi-ties outside their home country are eligible for coverage. For benefits listed in the Schedule of Benefits, this Insurance does not cover: ꔀPre-Existing conditions, defined as any Injury or Illness which meetscoverage under the Policy.ꔀSuicide or any attempt thereof, while sane or self destruction orꔀAny consequence, whether directly or indirectly, proximately orremotely occasioned by, contributed to by, or traceable to, or aris-ing in connection witha)war, invasion, act of foreign enemy hos-civil war; or b) mutiny, riot, strike, military or popular uprisingrection, rebellion, revolution, military or usurped power. ꔀThe refusal of a Physician or Hospital to make all medical reportsꔀCosmetic or plastic Surgery, except as the result of a covered acci-dent; for the purposes of the Policy, treatment of a deviated nasalꔀElective Surgery or Elective Treatment which can be postponeduntil the Insured Person returns to his/her Home County, where thebjective of the trip is to seek medical advice, treatment or Surgery.ꔀTreatment in connection with alcoholism and drug addiction, ordirected by a Physician for a condition which is covered hereunder.ꔀCongenital abnormalities and conditions arising out of or result-ꔀExpenses as a result or in connection with intentionally self-ꔀInjury sustained while taking part in mountaineering where ropesꔀDental care, except as the result of Injury to natural teeth causedꔀRoutine Dental Treatment.ꔀDrug, treatment or procedure that either promotes or preventstility or impotency, ster-dent pilot, operator or crew member, in or on, boarding or alight- Credit card enr203203 PARTICIPANT CONTACT INFORMATION: T__________________________ Female Male Date of birth ________/________/________ PROGRAM INFORMATION: U.S. institution where enrolled as student if applicableif ap
4 plicable Institution sponsoring study ab
plicable Institution sponsoring study abroad program if applicableif applicable Name of international institution you will attend____________________________________________________Host country _________________________Program start date ________/________/________Program end date ________/________/________ ENROLLMENT INFORMATION: I want my insurance to begin ________/________/________and continue for ________ months maximum 12 whole months onlymaximum 12 whole months only STUDYABROADPLAN ENROLLMENTFORM nroll on-line at www.culturalinsurance.com. 12/06 Basic Plan Rate (see Premium Rates section) $_________ x ________ mon whole months onlywhole months only = $__________ Total premiums= $__________ BeneficiaryÕs name________________________________________________ Relationship_____________________________ PAYMENT INFORMATION: Check/money order enclosed Visa MasterCard Please provide the following additional information for credit card payments:CardholderÕplease printplease printIhave read and understand the terms and conditions of the policy and authorize payment for the above enrollment. ocessing. All insurance materials are sent via standard U.S. Mail. Make checks payable (U.S.funds only) toCISIand mail with completed enrollment form to :CISI, River Plaza, 9 West Broad Street, Stamford, CT 06905-3788. Please contact CISIif you have any questions about this form or the policy. mm dd yymm dd yymm dd yymm dd yymm dd yymm yy Policy terms and conditions are briefly outlined in this document. A complete description is containedin the Plan of Insurance which you will receive after your enrollment. For office use only Participant ID# Premium Rates Basic Plan Monthly premium up to 25$3426-305141-6014661+261 Upgrade Plan MonthsAdditional premium 1-6$100*7-12200* Rates are valid until December 31, 2007. Full months only, please. CISICISI River Plaza ¥ 9 West Broad Street ¥ Stamford, CT 06902-3788 203-399-5121 ¥ www.culturalinsurance.com Cultural InsuranceServices International SCHEDULE OF BENEFITSBasic Plan Coverages Maximum limits ꔀper Accident or Sicknessper Accident or SicknessDeductible$100 ꔀAccidental Death and Dismemberment$10,000ꔀMedical Evacuation/Repatriation/ Combined limit $50,000 ꔀTeam Assist Plan CoveragesMaximum limits ꔀper Accident or Sicknessper Accident or Sickness $100,000 at 100% ꔀMedical Evacuation/Repatriation/ Combined limit $50,000 Team Assist Baggage Loss$1,000 $50 deductible; $100 per arexcept for cameras $250except for cameras $250 Emergency Medical Reunion$1,500 uition Refund50% up to 11/06 An application of insurancefor U.S. students studying abroad ed by CISICISIRiver Plaza ¥9 West Broad Street ¥ Stamfor203203www.culturalinsurance.com ¥ cisiwebadmin@culturalinsurance.com other offices Bonn ¥ Cape Town ¥ London ¥ Paris The Basic Plan and the Plan are underwritten by The Insurance Company of the State of Pennsylvania World Class Study Abroad