
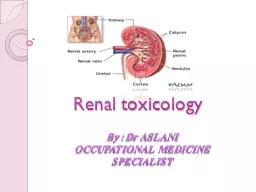
OCCUPATIONAL MEDICINE SPECIALIST PHYSIOLOGY Regulation of electrolytes Maintenance of acidbase balance Regulation of BP Remove wastes from the blood Reabsorption of H2OGAA Produce hormones ID: 777384
Download The PPT/PDF document "Renal toxicology By : Dr ASLANI" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


Slide1
Renal toxicology
By : Dr ASLANIOCCUPATIONAL MEDICINE SPECIALIST
Slide2PHYSIOLOGY
Slide3Regulation of electrolytes
Maintenance of acid-base balanceRegulation of BP Remove wastes from the bloodReabsorption of H2O,G,AA
Produce hormones
Function
Slide4Introduction
True incidence of CKD due to occupational & environmental exposure is unknown.Kidney is especially vulnerable to these exposures & toxins can be concentrated in kidney.These exposure are preventable causes of CKD.
Slide5Kidney Diseases
DurationAcute(Weeks)Chronic(Years)LocationGlomerular
Non-
glomerular
(tubular , interstitial)
The most common site of injury for toxicants is the proximal tubule.
Aghaee2a@gmail.com
5
Slide6Diagnosis
HistoryPhysical examinationClinical presentation of the renal diseaseMonitoring of exposed workers:lack of sensitive and specific testsSerial measurement Cr & BUN
Slide7Clinical history
Exposure histories: FrequencyIntensityPersonal protection
Slide8Clinical history & physical examination
Factors that enhancing nephrotoxicity:AgeGeneticHTNDiabetesGoutPre-exiting chronic renal disease
Slide9Hematuria
: Urinary tract cancerPapillary necrosis
GN
Proteinuria
:
HMW
Proteinuria
(
albuminuria
)
LMW proteinuria (β2-microglobulin & RBP)
Slide10Diagnostic Test
(U.S. Department of Health )correlate with site of possible damage & detect early renal tubular damage .glomerular injury (urine albumin)proximal tubule damage (RBP, glucosaminidase
,
alanine
amino peptidase)
distal tubule injury
(
osmolality
)
Slide11Slide12Limitations
unstable at certain urine pHsreturn to normal levels despite renal damagelarge inter-individual variationspredictive value of these newer tests has not been validated.
Slide13Clinical presentation
Acute renal failure: ATNChronic renal failure: Chronic interstitial nephritis
Slide14Acute renal dysfunction
Usually after high-dose exposurerenal lesion : ATNextra renal manifestations usually dominateclinical presentation, course of ARF are very similar in all exposures.
Slide15ATN
Hours to days after exp: urine output< 500 ml/d. The urine analysis: renal tubular cells, muddy brown granular casts, Pr, RBC,WBC or casts of either cell type: NegBUN ,Cr and electrolyte abnormalities After 1-2 weeks: diuresis
Slide16ATN
TreatmentHemodialysis and/or hemoperfiision have almost no role in accelerating the clearance of occupational and environmental toxins. These techniques are effective: certain alcohols, salicylate, lithium, theophylline
Slide17ARF caused
by heavy metalsDivalent metals, Cr, Cd, Hg & vanadiumExposure: welding cadmium-plated metalsExposure to Cd fumes → cough & progressive pulmonary distress to ARDS RF in form of ATN Bilateral cortical necrosis in severe exposure
Slide18ARF
caused by organic solventsRoute of absorption: lungs (most common), skinLipophilic & distribute in: fat, liver, BM, blood, brain & kidney
Slide19Organic
solventsA) halogenated Hydrocarbons carbon tetrachloride (CCL4): - Acute exposure: - CNS GI -after 7-10d :↓urine output, prerenal azotemia
Slide20Organic
solvents Other aliphatic halogenated hydrocarbons: 1-ethylene dichloride (C2H4Cl2): --less potent than CCl4 as a renal toxicant but greater CNS toxicity 2-Chloroform (CCl3H): --more nephrotoxic than CCl4 3-Trichloroethylene (C2HCl3):-- cleaning agent4-Tetrachloroethane (C2H2Cl4):--most toxic of halogenated hydrocarbons
5- Ethylene chlorohydrin
--penetrates the skin readily and is absorbed through rubber gloves
Slide21B)
Nonhalogenated hydrocarbons : 1-Dioxane: less toxic than halogenated hydrocarbons2 -Toluene: -- reversible ATN due to toluene inhalation (glue-sniffing)3- Ethylene Glycol:
--Mono ethyl ether, mono methyl , butyl ether
--irritants of skin and mucous membranes, CNS depressants.
4-phenol (carbolic acid):
--Local burns, dark urine
Slide22ARF caused
by Arsinesemiconductor industryPrimarily hemotoxic Firs sign immediately or after a delay up to 24h:malaise, abd cramps, nausea, vomitingRF due to ATN secondary to hemoglobinuriaHydration, manitol
Exchange transfusion to prevent further
hemolysis
Slide23Chronic kidney diseases caused by lead
Exposure: ingestion of leaded paint, battery manufacturing, mining, combustion of leaded gasolineAbsorbed by GI (adults:10% , children:50%) & lungsConcentrated in bone (90%) & kidneys Chronic lead exposure→ ( fanconi-type syndrome) After 5-30y : progressive tubular atrophy & interstitial fibrosis
Slide24Cont,…
Mechanisms of gout : 1-↓urine clearance of uric acid 2- crystallization at low urate concentration 3- lead-induced formation of guanine crystalsMechanisms of HTN:
acute lead intoxication
1-↑ intracellular Ca
2-inhibition Na+,K+ ATPase
3-direct vasoconstriction
4-alteration in RAA axis
Slide25Classic
presentation of lead nephropathy:CKD+ HTN+ gout. CKD+ low-grade proteinuria , ( without gout or HTN )U/A 24 hr: 1-2 g Ultrasonography :small, contracted kidneysRenal biopsy :tubular atrophy, interstitial fibrosis, and minimal inflammatory infiltrates.
Electron
microscopy
:
intranuclear
inclusion bodies usually are present in the early stages of lead exposure but often are absent after chronic exposure or after lead
chelation
.
Cont,…
Slide26Diagnosis :
Measuring blood lead levelEDTA lead mobilization testTibial K x-ray fluorescence correlate with bone leadCont,…
Slide27Exposure:Cd
-sulfide in ores of zinc, lead, and copper.nickel-cadmium batteries, pigments, glass, metal alloys, and electrical equipment.40% - 80% of Cd is stored in: liver, kidneys (1/3) Cd is a contaminant of tobacco smoke. Only 25% of ingested Cd is absorbed. Chronic kidney diseases caused by cadmium
Slide28Cd blood rises then falls because it taken by the liver.
RBC & soft tissues: Cd-metallothionein.This complex is filtered at the glomerulus, undergoes endocytosis in the prox.T, and is later degraded in the lysosomes. The adverse effects of Cd on the Prox.T:
Unbound
Cd
, that interfere with zinc-dependent enzymes.
Cont,…
Slide29Target organs : kidney & lung
fanconi syndromeHypercalciuria with normocalcemia, hyperphosphaturia→ osteomalacia, pseudofx, nephrolithiasisUretral colic from calculi in 40%Itai-itai dx : painful bone dx with pseudofx in japanCont,…
Slide30Possible causes of osteomalacia:
1- a direct effect of cd on bone 2- ↓renal tubular reabsoroption of Ca & P 3- ↑PTH & ↓ hydroxylation of vit DCont,…
Slide31Renal cadmium toxicity low-molecular-weight
proteinuriaurinary calculimultiple tubular abnormalitiesCd urine >10 µg/g Treatment :except removal from the exposure treatment of osteomalaciaCont,…
Slide32Chronic kidney diseases caused by mercury
Exp: Inhalational of Metal fume & ingestion1- ATN 2-Nephrotic syndromemercury exposure:Membranous nephropathyminimal-change diseaseanti-GBM
Slide33Clinical presentation of ATN: extrarenal manifestations Dx
: history of exposureglomerular disease such as membranous nephropathy??blood and urine mercury concentrations do not correlate with renal disease. Spontaneous resolution of the proteinuria following removal from the source of mercury exposure is consistent with mercury-mediated glomerular disease.Cont,…
Slide34Beryllium
Exposure: manufacture of electronic tubesfluorescent light bulbsmetal foundriesAbsorption: inhalation
Slide35manifestation of
berylliosis :systemic granulomatous disease: lungs, bone, bone marrow, liver, lymph nodes, …kidneys:granulomas and interstitial fibrosis. Hypercalciuria, Hyperuricemia ,urinary tract stones.(30%) PTH depressed,Cont,…
Slide36Reproductive Toxicity
Slide37Reproductive Toxicity
Reproductive functionWomen Who Are PregnantWomen of Child Bearing AgeMen
Slide38Male:
Spermatogonium spermatocyte spermatid mature spermatozoa (3 months)
Slide39Hormonal disorder
Hormonal & semen disorderOligospermia
Azoospermia
Asthenospermia
&
teratospermia
Asthenospermia
&
oligospermia
Adverse Male Reproductive
Effects
Slide40Female:
Embryonic
Fetal
Prenatal
death
Major
malformation
Minor malformation
Functional defects
1-2w
8w
Slide41Difficulty in studying
reproductive toxicity in womennature of the female cyclerelative frequency spontaneous abortions
common occurrence of birth defects in general population
Slide42Infertility:
Mens dis:LBW (< 2500 gr):Adverse Female Reproductive Effects
Slide43Birth defects:
Preterm (<37wk):SAB (fetal loss 20 wk ):
Slide44Slide45Slide46The
end