
Topic 1 Basic nutritional assessment SubSaharan Africa Nursing Network Objectives By the end of this session participants should be able to Identify the common required anthropometric measurements in paediatric oncology ID: 1007255
Download Presentation The PPT/PDF document "Module 9: Nutritional support for childr..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




1. Module 9: Nutritional support for children with cancerTopic 1: Basic nutritional assessmentSub-Saharan Africa Nursing Network
2. ObjectivesBy the end of this session, participants shouldbe able to:Identify the common required anthropometric measurements in paediatric oncologyIdentify and flag sub-optimal anthropometricsConduct a diet review
3. WeightIt is important to check the weight of the patient at every appointment.On first admission Used alone, or in combination with the height to calculate doses of chemotherapyDaily weight check helps assess reduction in tumour mass, nutrition, and hydration statusWith subsequent visits Gives an indication of appetite or elimination, which may be a side effect of chemotherapy or a co-morbidity (physical or psychological).Chemotherapy dose may need to be adjusted for weight loss/gain
4. HeightUsed to calculate the body surface area(BSA).BSA is the parameter mostly used forchemotherapy dose calculation.Used to monitor growth
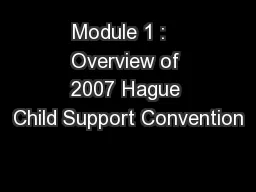
5. Weight for height ratioReflects body weight in relation to heightImportant to plot values for each child on growth curves and compare changes in the child over timeCan be indicative of acute malnutrition (wasting) versus chronic malnutrition (stunted growth)
6. Weight for height ratio
7. Body surface area (BSA)Required for calculation of drug doses andfluid requirementsBSA Children less than 10Kg, all doses calculated using BSA are usually reduced or calculated as mg/Kg
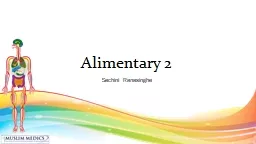
8. Mid arm circumference/ Triceps skin fold (MUAC tapes/skinfold callipers)Measurements for monitoring of muscle mass and body fat
9.
10.
11. Factors affecting accuracyTechniqueEquipmentLevel of cooperation from the patient>> It is necessary to repeat measurementsand remove outliers when comparing readingsover time.
12. Benefits of anthropometricmeasurements to nutritional statusTo identify patients at nutritional riskAssess efficacy of nutritional supportIdentify patients who require dietary counsellingIdentify patients who require nutritional interventionIt is important to assess at time of diagnosis and repeatedly over time, to see changes
13. Food historyIt is important to note what the patient is eating. This helps provide an indication of their nutritional status.A 24 hour diet recall is usually used for obtaining information on the food, energy and nutrient intake of a child.Ask the family to enumerate every thing the child has eaten in the last 24 hours.Through the classes of food listed, nutrient deficits could be anticipated and corrected and a nutritional and an education plan put in place with the child and family.
14. Nutritional needsProtein and calorie needs typically increasein children with cancer because ofphysiological stressThe amount of energy required to maintain normal homeostatic function at rest (resting energy expenditure) is higher for children with cancer.Nurses play an important role in anticipatingrisk factors, assessing nutritional status, and initiating prompt interventions.
15. Nutritionally at-risk patientsWt. loss of 5% or more of pre-illness body weight.Weight-for-height <10th percentile for age.Voluntary food intake <70% of estimated requirements for 5 or more days.Anticipated GIT dysfunction for more than 5 days.These patients require immediate nutritional support and referral to a nutritionist (if available) and prompt nutritional intervention.
16. Nutritional interventions 1Goal is to prevent or reverse malnutritionSymptom relief: Managing some side effects of treatment will prevent or reverse nutrition problems e.g. nausea and vomiting, mucositis, constipationDietary adaptation: in terms of likes, frequency, quantity, proportion of food classes(e.g. more caloric)Parent/family teaching Appetite stimulation
17. Nutritional interventions 2If the child does not manage to achieve adequate nutritional intake then additional interventions may be needed:Artificial supplement feeds: e.g. F75, F100Nasogastric feedingOther enteral feed such as by gastrostomyTotal parenteral nutrition where available
18. AssessmentWhat is the anthropometric measurement commonly used for drug dosing in paediatric oncology?State two other uses of anthropometric measurements.What is the equipment used for measuring triceps skinfold?
19. ContributorsMarilyn J Hockenberry PhD, RN, FAANTexas Children’s Hospital, Houston, Texas, USAEnyo Asi BosumprahKorle-Bu Teaching Hospital, Accra, GhanaMpho Thabang M. RaletshegwanaPrincess Marina Hospital, Gaborone, BotswanaRachel Hollis FRCNWorld Child Cancer, UKNdagire MariamUganda Cancer Institute, Kampala, UgandaBiemba K Maliti Cancer Diseases Hospital, Lusaka, ZambiaColleen Nixon, MSN, RN, CPHON®Boston Children's Hospital, Boston, USAElianeth A. Kiteni RN, BScN, PGD M&EMuhimbili National Hospital, TanzaniaElizabeth Mtunga, RN BSN CPHONKilimanjaro Christian Medical Centre, TanzaniaLiz Sniderman, MSN APRN CPNP-AC CPHON St. Jude Children’s Research Hospital | St. Jude Global, Memphis, Tennessee, USAGlenn Mbah Afungchwi, PhD MPH RNMbingo Baptist Hospital/ World Child Cancer, Cameroon.
20. Acknowledgements