
v1 Page 1 of 16 Did you print this document yourself The Trust discourages the retention of hard copies of policies and can only guarantee reasons you need to print a policy off it is only valid ID: 942365
Download Pdf The PPT/PDF document "Paracentesis for Malignant Ascites Proce..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



v.1 Page 1 of 16 Paracentesis for Malignant Ascites Procedure Did you print this document yourself? The Trust discourages the retention of hard copies of policies and can only guarantee reasons, you need to print a policy off, it is only valid for 24 hours. Author/reviewer: (this version) Dr Anne-marie Carey - Consultant Palliative Medicine Lesley Barnett - Lead Can
cer Nurse Date written/revised: November 2012 v.1 Page 3 of 16 1 Introduction 4 2 Purpose and Scope 4 3 Responsibilities, Duties and Accountabilities 5 4 Paracentesis 5 4.4 Complications of paracentesis 5 Training implications/Support 11 6 Monitoring Compliance with the Procedural Document 12 7 Definitions 12 8 Equality Impact Assessment 12 9 Associ
ated Trust Procedural Documents 13 10 References & Acknowledgement 13 Appendix 1 Equipment r Appendix 2 PleurX Drains 16 v.1 Page 5 of 16 3. DUTIES AND RESPONSIBILITIES 3.1 The overall responsibility for the organisation lies with The Chief Executive of DBH ng and medical staff are accountable for their own actions and omissions and must apply their knowledg
e and skills at all 3.2 Registered nurses and doctors have a their required competencies. Report near-rious incidents in relationship to a paracentesis procedure (as per NMC and GMC guidance). 3.3 The Managing Director of Doncaster Commu 4. PROCEDURE - PARACENTESIS Paracentesis may not be appropriate if the prognosis is very short and the patient is rapidly deteriorating.
If the prognosis is very short but patient has troublesome ed to reduce discomfort. Ideally the patient should be admitted asUncomplicated follow up procedures may be 4.1 Type of ascites: Transudates are usually seen in unlikely to be helpful.albumin gradient (SAAG) can be ta 4.2 Indications for procedure: Pain, discomfort or tightness due to v.1 Page 7 of 16 I
f there is ascites clinically, or it is will be limited. 4.5.2 Blood tests In order to proceed with a safe paracentesis, the following should be considered its outweigh the risks, paracentesis can these cases, the patient should be A platelet count and clotting screen s/L to safely proceed. A serum albumin and U&E should be taken if: More than 4-6 litres is to be remo The p
atient is clinically dehydrated, or The patient has reacted badly to previous paracentesiswith: Risk of haemorrhage. Consider the use of vitamin K to normalise the INR before Risk of haemorrhage Significant anaemiaMay be worsened by haemorrhage, lower reserves for coping with procedure. May make correct attribution of symptoms more difficult. Low sodium (less than 126)Po
or prognostic indicator. Paracentesis can cause further electrolyte disturbance Paracentesis can cause further electrolyte disturbance Lower reserves for dealing with fluid shift Lower reserves for dealing with fluid shift, may be associated with raised INR Low protein and albumin (less than 20)Likely to re-accumulate more quickly due to low oncotic pressure (production r
ate significant intravascular depletion Low white cell count / neutropenia Risk of infection 4.6 Diuretics a prognosis of several months as it fluid. Consider them where the serum ascites albu�min gradient (SAAG) is 11g/L.spironolactone is 60% at 300mg. The patients most likely to respond to diuretic v.1 Page 9 of 16 est slightly raised To allow gravity
to assist in the drainage Confirm once again the prThe usual site for paracentesis is the left side10cm from midline or supra-pubically avoid scars, tumour masses, distended liver inferior epigastric artery that runs either side of the midline Guided by ultrasound marking Usual sites for paracentesis, To minimise risk of complications such as perforation and haemorr
hage Action Rationale Clean the area with sterile solution e.g. chlorhexidine 2% To minimise the risk of infection roughout To minimise the risk of infection injection into the area to be cannulated. Start subcutaneously and gradually infiltrate deeper until fluid is aspirated from the peritoneal cavity. Wait 3 minutesreports numbness on testing with a needle For patient
comfort and to aid cooperation with the procedure whether it is safe to proceedIf there is any concern re safety of proceeding stop and review confirm presence and site of Insert large bore needle, cannula or Bonanno catheter into the peritoneal cavity. A scalpel is rarely required At this point a sample can be taken for protein and albumin levels if required Apply a draina
ble catheter bag To collect and measure the ascitic fluid Apply an adhesive dressing to the catheter if To prevent it from becoming dislodged. v.1 Page 12 of 16 6. MONITORING COMPLIANCE WITH THE PROCEDURAL DOCUMENT What is being Who will carry out How often How Reviewed/ Specialist Palliative Care Consultant procedures Specialist Palliative Care Consultan
t/ developed to address. Complications Specialist Palliative Care Consultant/ developed to address. 7. DEFINITIONS such as cancer, cirrhosis of the liver, congestive cardiac failurstomach, pancreas and bronchus. Paracentesisll volume paracentesis) or as an inpatient. Removal of more than 4-6 litres increases but may give symptom relief for longer until 8. EQUALITY
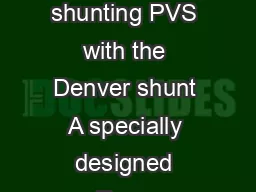
IMPACT ASSESSMENT An Equality Impact Assessment (EIA) has the Equality Analysis Policy (CORP/EMP 27) and the Fair v.1 Page 14 of 16 Guidelines for the Management www.palliativedrugs.com Guidelines for the Managementwww.palliativedrugs.com v.1 Page 16 of 16 APPENDIX 2 PleurX Drains For some patients with large volume recurrentPossible advantages of usi
ng Pleurx to manage recurrent malignant ascites: Avoids the need for repeat needle drainage procedures (paracentesis). Less visits to hospital and reduced hospital length of stay. Home management Prevents large build-up of fluid as you can dr Pleurx is usually well tolerated and has few complications. drainage procedures which can take longer periods of time and restri