
Isolated fetal choroid plexus cysts Society of Maternal Fetal Medicine with the assistance of Karin M Fuchs MD Published in Contemporary OBGYN April 2013 IncidenceDefinition ID: 914106
Download Presentation The PPT/PDF document "SMFM Clinical Practice Guidelines" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






Slide1
SMFM Clinical Practice Guidelines
Isolated fetal choroid plexus cysts
Society of Maternal Fetal Medicine with the assistance of Karin M. Fuchs MD
Published in
Contemporary OB/GYN /
April
2013
Slide2Incidence/Definition
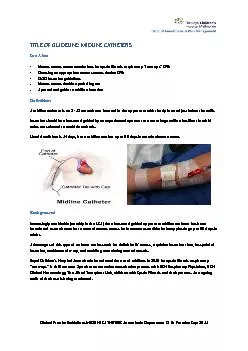
A choroid plexus cyst is a small fluid-filled structure within the choroid of the lateral ventricles of the fetal brain. Sonographically
, choroid plexus cysts appear as echolucent cysts within the echogenic choroid. Choroid plexus cysts may be single or multiple, unilateral or bilateral, and most often are less than 1 cm in diameter. Choroid plexus cysts are identified in approximately 1% to 2% of fetuses in the second trimester and they occur equally in male and female fetuses
Slide3Major clinical implications of an isolated choroid plexusWhen a choroid plexus cyst is identified, the presence of structural malformations and other
sonographic markers of aneuploidy should be assessed with a detailed fetal anatomic survey.Detailed examination of the fetal heart (4-chamber view and outflow tracts view) and hands (for “clenching” or other abnormal positioning) should be included, as well as fetal biometry for assessment of intrauterine growth restriction.
Slide4Major clinical implications of an isolated choroid plexus
A choroid plexus cyst is not considered a structural or functional brain abnormality. Most choroid plexus cysts are isolated and occur in otherwise low-risk pregnancies.The only association of some significance between an isolated choroid plexus cyst and a possible fetal problem is with trisomy 18.
Choroid plexus cysts are present in 30% to 50% of fetuses with trisomy 18. When a fetus is affected by trisomy 18, multiple structural anomalies are almost always evident, including structural heart defects, clenched hands, talipes deformity of the feet, growth restriction, and polyhydramnios. When a structural anomaly is present in addition to choroid plexus cysts, the probability of trisomy 18 is 37%.In the absence of associated
sonographic
abnormalities, the likelihood of trisomy 18 is extremely low in otherwise low-risk pregnancies.
Slide5Counseling
Counseling for a woman after prenatal identification of a fetal choroid plexus cyst should be guided by the presence or absence of other sonographic markers or structural abnormalities, results of maternal screening for risk of trisomy 18 (if performed), and maternal age
Slide6Follow up
More than 90% of choroid plexus cysts resolve, most often by 28 weeks.Studies evaluating neurodevelopmental outcomes in
euploid children born after a prenatal diagnosis of choroid plexus cysts have not shown differences in neurocognitive ability, motor function, or behavior. Therefore, neither serial antenatal ultrasounds nor post-natal evaluation are clinically useful.
Slide7The practice of medicine continues to evolve, and individual circumstances will vary. This opinion reflects information available at the time of its submission for publication and is neither designed nor intended to establish an exclusive standard of perinatal care. This presentation is
not expected to reflect the opinions of all members of the Society for Maternal-Fetal Medicine.
These slides are for personal, non-commercial and educational use onlyDisclaimer
Slide8DisclosuresThis opinion was developed by
the Publications Committee of the Society for Maternal Fetal Medicine with the assistance of Stanley M. Berry,
MD, Joanne Stone, MD, Mary Norton, MD, Donna Johnson, MD, and Vincenzo Berghella, MD, and was approved by the executive committee of the society on March 11, 2012. Dr Berghella and each member of the publications committee (Vincenzo Berghella, MD [chair], Sean Blackwell
, MD [vice-chair],
Brenna Anderson
, MD, Suneet P. Chauhan,
MD, Jodi
Dashe, MD, Cynthia
Gyamfi-Bannerman, MD, Donna
Johnson
, MD
,
Sarah Little
, MD, Kate Menard, MD,
Mary Norton
, MD, George Saade, MD,
Neil Silverman
, MD, Hyagriv Simhan,
MD,
Joanne
Stone, MD, Alan Tita,
MD,
Michael
Varner, MD) have submitted
a conflict
of interest disclosure
delineating
personal, professional, and/or
business interests
that might be perceived as a
real or
potential conflict of interest in
relation to
this publication.