
Dr Tan Jiunn Liang Clinical Specialist Respiratory Medicine Department of Medicine Universiti Malaya Medical Centre Disclaimer This program is provided as a service to the medical profession and represents the opinions of the speakers not necessarily those of Merck or MSD or its affil ID: 709771
Download Presentation The PPT/PDF document "Raising the Bar in the Management of Adv..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Raising the Bar in the Management of Advanced/Metastatic NSCLC
Dr Tan Jiunn LiangClinical Specialist (Respiratory Medicine)Department of MedicineUniversiti Malaya Medical CentreSlide2
Disclaimer
This program is provided as a service to the medical profession and represents the opinions of the speakers, not necessarily those of Merck or MSD or its affiliatesMerck or MSD or its affiliates do not recommend the use of any product in any manner different from that described in the prescribing informationDue to individual countries' regulatory requirements, approved indications and uses of products may vary
Before prescribing any products, please consult the local prescribing information available from the manufacturer(s)Slide3
Outline
Overview of NSCLCChanging therapeutic landscape for NSCLCImmunotherapyDevelopmentMechanism (in brief)Clinical trialsFuture of lung cancer treatmentTake home message (Summary)Slide4
Lung Cancer Remains a Major Global Health Burden
One of the most common cancers and leading cause of cancer deaths in US and worldwide[1,2] New cases, 2017 (estimated): US, 222,500; global, 1.8 million Deaths, 2017 (estimated): US, 155,870; global, 1.6 million
~ 80% to 85% of cases are NSCLC (~ 184,000)[3]Stage IV at diagnosis: ~ 57%[4]Represented by multiple disease subtypes[5]Standard of care for stage IV NSCLC: systemic therapy
1. GLOBOCAN Cancer Fact Sheets. 2012. 2.
Siegel RL, et al. CA Cancer
J Clin. 2016;66:7-30. 3. American Cancer Society. Non-small-cell Lung Cancer. 4. SEER Cancer Statistics Review, 1975-2002. 5. Li T, et al. J Clin Oncol. 2013;31:1039-1049.Slide5
Overall Survival in Lung cancer
"Overall survival, expressed as median survival time (MST) and 5-year survival, by pathologic stage using sixth edition of TNM (A) and proposed International Association of the Study of Lung Cancer
recommendations.Slide6
Lung cancer = end of the road?Slide7
?Slide8
Li T, et al. J Clin Oncol. 2013;31:1039-1049.
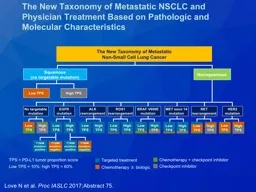
NSCLC Evolution: From Single Disease to Many Molecularly-Defined Subsets
NSCLC
as one disease
Histology-Based Subtyping
Squamous
34%
Other
11%
Adenoca
55%
Adenocarcinoma
Squamous Cell Cancer
ALK
HER2
BRAF
PIK3CA
AKT1
MAP2K1
NRAS
ROS1
RET
EGFR
KRAS
Unknown
EGFRvIII
PI3KCA
EGFR
DDR2
FGFR1 Amp
Unknown
First-targeted tx
ALK
EGFRSlide9
Therapeutic Decision Making
Histologic
Subtyping
Genotyping for
Predictive Biomarkers
Adapted from Gandara DR, et al. Clin Lung Cancer. 2009;10:392-394.
Decision Making for Advanced NSCLCSlide10
Histologically Distinct Subtypes of NSCLC
American Cancer Society. Non-small-cell lung cancer.
Rekhtman N, et al. Mod Pathol. 2011;24:1348-1359.
Slide11
Changes in the Therapeutic Landscape of Stage IV Lung CancerSlide12
Changes in the Therapeutic Landscape of Stage IV Lung CancerSlide13
Personalized Therapy in Advanced-Stage NSCLC: Current Therapeutic Landscape
Chemotherapy
Checkpoint Inhibitors
Targeted TKI Therapy
EGFR
ALK
ROS1
BRAF
V600E
MET amp
HER2
MEK
Histologic
subtype
Anti–PD-1
Anti–PD-L1
Anti-CTLA4
1970s - today
2000s - today
2015 - todaySlide14
Multidisciplinary Integration of Biomarker Testing in Advanced NSCLC
Adapted from: Gandara D, et al. ASTRO/ASCO/IASLC
Symposium on Molecular Testing. 2012.
Pulmonologist
Interventional radiologist
Surgeon
Pathologist
Oncologist
Pulmunologist
Multidisciplinary
team
(
tumour
board)
Referring physician
Med oncologist
Thoracic surgeon
Radiation oncologist Pulmonologist
Radiologist
Pathologist
Goal:
Identify
“actionable” oncogenes
Identify pt
Identify
target
lesion
Biopsy
Histology evaluation
Molecular biomarker testing
Determine
therapy
Progression
r
ebiopsy
Determine
new therapy
Progression
r
ebiopsy
Treat
TreatSlide15
Frequency
of Driver Mutations in NSCLC, %
AKT1
1
ALK
3-7
BRAF
1-3
EGFR
10-35
HER2
2-4
KRAS
15-25
MEK1
1
NRAS
1
PIK3CA
1-3
RET
1
ROS1
1
BRAF
HER2
MEK1
AKT1
ALK
PIK3CA
NRAS
ROS1
RET
www.mycancergenome.org.
Molecular Subsets of Lung Cancer Defined
by Driver Mutations
Unknown
KRAS
EGFRSlide16
Targeted Therapy for Adenocarcinoma
Tsao AS, et al. J Thorac Oncol. 2016;11:613-638.Slide17
Considerations for First-line Therapy of Advanced NSCLC
Clinical featuresPerformance statusComorbidities/smoking status
HemoptysisCNS metastasesPrevious chemotherapy in adjuvant or locally advanced settingHistologic subtypingAdenocarcinoma, squamous, other
Molecular subtyping EGFR mutation, ALK/ROS1
PDL-1Slide18
Adapted from Gandara DR, et al. Clin Lung Cancer. 2012;13:321-325.
Maintenance Options After Platinum-Based Therapy With Nonprogressive NSCLCSlide19
Progression to Next Line of Therapy in NSCLCSlide20
Number of Treatment Options over Time for Selected Tumors (1996–2016)Slide21Slide22
“Tumour immunology has long had a bright future”
“For those mice in the audience, it’s good news...”
“Immunotherapy earns its spot in the ranks of cancer therapy”
“…a tipping point in the fight against cancer”
Cancer ImmunotherapySlide23
Cancer Immunotherapy in the newsSlide24
History of Immunotherapy
Elert
E. Nature. 2013;504:S2-S3.
1796: First use of immunotherapy,
Jenner smallpox vaccine
1976: BCG vaccine for bladder cancer
1863: Connection between immunotherapy and cancer recognized
1985: Interferon first approved for hairy cell leukemia
1992: IL-2 approved for RCC
1997: First mAb for cancer approved, rituximab
2008: First cancer vaccine approved for RCC
2010:
Sipuleucel
-T approved for prostate cancer
2011: CTLA-4 inhibitor approved for melanoma
2014-2015: PD-1 inhibitors approved for melanoma, squamous NSCLC
2015: First oncolytic virus approved for melanoma
2016: PD-1 inhibitor approved for cHL
PD-L1 inhibitor approved for UCSlide25
Immune System Function and Immune Response
Janeway
CA Jr, et al.
Immunobiology
: the immune system in health and disease. 2001.
Innate Immunity
Adaptive Immunity
Identify and destroy foreign or abnormal cells in the body
Nonspecific
First line of defense
WBCs (natural killer cells, neutrophils)
Activation of adaptive response
Specific
Adapts specifically to diverse stimuli
B-cell antibody production
T-cell stimulation
Memory functions
Dendritic cell
Mast cell
Macrophage
Natural
killer cell
Natural
killer T cell
B cell
T cell
CD4+
T cell
CD8+
T cell
Antibodies
λ
δ
T cell
Complement
protein
Neutrophil
Eosinophil
Basophil
Granulocytes
Goal of immunotherapy for cancer: to
“
educate and liberate
”
underlying anticancer immune responses
Tumor-associated antigens can be identified by the immune system and
destroyedSlide26
The tumour microenvironment
Hallmarks of Cancer: The Next Generation Douglas
Hanahan
, Robert A. Weinberg. Cell
Vol
144, Issue 5, p646–674, 4 March 2011Slide27
CTLA-4 and PD-1/PD-L1 Checkpoint Blockade for Cancer Treatment
Ribas
A. N
Engl
J Med. 2012;366:2517-2519.
Interfering with these receptor/ligand systems restores antitumor immunitySlide28Slide29
History of Cancer Immunotherapy: Key Milestones
IFN-
α
as adjuvant
therapy for melanoma
[2]
Immune component
to spontaneous regressions in melanoma
Adoptive T-cell immunotherapy
IL-2 approved
for RCC and
melanoma (US)
[3,4]
First immunotherapy approved for prostate cancer (sipuleucel-T)
[8]
First checkpoint
inhibitor (ipilimumab)
approved for advanced melanoma
[9]
2000s
First tumor-associated antigen cloned (MAGE-1)
BCG
approved
for bladder
cancer
Discovery of checkpoint inhibitors
[5-7]
Discovery of
dendritic cell
[1]
Tumor-specific
monoclonal Abs
Pembrolizumab and nivolumab approved for advanced melanoma
[10,11]
1970s
1980s
1990s
2011
2014
2015
Nivolumab
approved for NSCLC
[12,13]
Pembrolizumab approved for
PD-L1+ NSCLC
[14]
Nivolumab approved for RCC
[15]
2016
Atezolizumab
granted
Priority Review for PD-L1+ NSCLC
Atezolizumab approved for advanced urothelial carcinoma
[16]
Nivolumab approved for HL
[17]Slide30
Chemotherapy vs standard treatment
Immunotherapy : durable responses in some patients
Melanoma, anti-CTLA-4
Melanoma, anti-CTLA-4 +/- anti-PD-1
Anti-CTLA-4
Control
NSCLC Meta-analysis, JCO, 2008
The potential for cureSlide31
Response Patterns for Immunotherapy Compared With Targeted Therapy
Ribas
A, et al.
Clin
Cancer Res. 2012;18:336-341.
Yrs
Immunotherapy
Targeted Therapy
Percent Alive
Percent Alive
1
2
3
0
1
2
3
0
YrsSlide32
Mutational Burden in Human Cancers
National Cancer Informatics Program.Slide33
Gene alteration in lung cancerSlide34
Immune Checkpoint Blockade
includes agents targeting the negative regulators CTLA-4 and PD-1CTLA-4 attenuates the early activation of naive and memory T cells in the lymph nodesinclude ipilimumab and tremelimumab
PD-1 modulates the effector phase of T cell activity in peripheral tissues via interaction with PD-L1 and PD-L2 include nivolumab and Pembrolizumab
Kyi C, et al. FEBS Lett. 2014;588:368-376Slide35
Clinical trials
Where it all started…Slide36
Pembrolizumab
KEYNOTE 001, 010, 021, 028 Slide37
Pembro
vs Doc in Previously Treated PD-L1+ NSCLC
Pts with advanced NSCLC PD after ≥ 2 cycles of platinum-doublet chemotherapy,
PD-L1 TPS ≥ 1%, ECOG PS 0-1, no brain metastases
(N = 1034)
Pembrolizumab 2 mg/kg Q3W
for 24 mos
(n = 345)
Docetaxel 75 mg/m
2
Q3W
per local guidelines
(n = 343)
Pembrolizumab 10 mg/kg Q3W
for 24 mos
(n = 346)
Stratified by ECOG PS (0 vs 1), region (east Asia vs not), PD-L1 TPS (≥ 50% vs 1% to 49%)
*In both the PD-L1 TPS
≥ 1% and ≥ 50% populations.
Herbst
RS, et al. Lancet. 2016;387:1540-1550.
KEYNOTE-010: NSCLC
Primary endpoints*: PFS, OS
Secondary endpoints: ORR, DoR, safety
TPS, tumor proportion score
.Slide38
All pts experienced OS benefit from pembrolizumab
Treatment Arm
Median OS,
Mos (95% CI)
1-Yr OS, %
HR vs Docetaxel
(95% CI);
P
Value
Pembro 2 mg/kg
10.4 (9.4-11.9)
43.2
0.71
(0.58-0.88); .0008
Pembro 10 mg/kg
12.7 (10.0-17.3)
52.3
0.61 (0.49-0.75); < .0001
Docetaxel
8.5 (7.5-9.8)
34.6
–
Treatment Arm
Median OS,
Mos (95% CI)
HR vs Docetaxel
(95% CI);
P
Value
Pembro 2 mg/kg
14.9 (10.4-NR)
0.54 (0.38-0.77); .0002
Pembro 10 mg/kg17.3 (11.8-NR)
0.50 (0.36-0.70); < .0001Docetaxel8.2 (6.4-10.7)–
PD-L1 TPS ≥ 50%
PD-L1 TPS ≥ 1%
100
80
60
40
20
0
5
0
10
15
20
25
OS (%)
Mos
100
80
60
40
20
0
5
0
10
15
20
25
OS (%)
Mos
Pembrolizumab 2 mg/kg
Pembrolizumab 10 mg/kg
Docetaxel
HR, 2 vs 10 mg/kg: 1.17
(95% CI: 0.94-1.45)
HR, 2 vs 10 mg/kg: 1.12
(95% CI: 0.77-1.62)
Herbst
RS, et al. Lancet. 2016;387:1540-1550.
KEYNOTE-010Slide39
OS by Pt Subgroups*
*Data for the pembrolizumab doses were pooled.
0.1
1
10
Overall
Sex
Male
Female
ECOG PS
0
1
Histology
Squamous
Adenocarcinoma
521/1033
332/634
189/399
149/348
367/678
128/222
333/708
0.67 (0.56-0.80)
0.65 (0.52-0.81)
0.69 (0.51-0.94)
0.73 (0.52-1.02)
0.63 (0.51-0.78)
0.74 (0.50-1.09)
0.63 (0.50-0.79)
Subgroup
Events/Pts, n
HR (95% CI)
Favors Pembrolizumab
Favors Docetaxel
PD-L1 tumor proportion score
³
50%
1% to 49%
204/442
317/591
0.53 (0.40-0.70)
0.76 (0.60-0.96)
Age
< 65 yrs
³
65 yrs
317/604
204/429
0.63 (0.50-0.79)
0.76 (0.57-1.02)
Tumor sample
Archival
New
266/455
255/578
0.70 (0.54-0.89)
0.64 (0.50-0.83)
EGFR
status
Mutant
Wild type
46/86
447/875
0.88 (0.45-1.70)
0.66 (0.55-0.80)
Herbst
RS, et al. Lancet. 2016;387:1540-1550.
KEYNOTE-010Slide40
ORR significantly higher with both 2 mg/kg and 10 mg/kg
pembrolizumab vs docetaxel regardless of PD-L1 TPS
Herbst RS, et al.
Lancet. 2015;[
Epub
ahead of print].
PD-L1 TPS ≥ 50%
PD-L1 TPS ≥ 1%
100
80
60
40
20
0
100
80
60
40
20
0
5
10
15
20
0
5
10
15
20
0
Response (%)
Response (%)
Mos
Mo
Pembrolizumab 2 mg/kg Pembrolizumab 10 mg/kg Docetaxel
Pembrolizumab 2 mg/kg
Pembrolizumab 10 mg/kg
Docetaxel
NR (4.2-10.5)
NR (4.2-12.5)
6 (2.7-6.1)
Median DoR, Mos (95% CI)
NR (4.2-10.4)
NR (4.4-12.6)
8 (2.6-8.3)
Median DoR, Mos (95% CI)
Pembrolizumab 2 mg/kg
Pembrolizumab 10 mg/kg
Docetaxel
KEYNOTE-010Slide41
Recently… in the news!
Reck
, Martin, et al. "
Pembrolizumab
versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer." New England Journal of Medicine (2016).Slide42
Benefit of pembrolizumab
was evident in all subgroups
KEYNOTE-024
Reck
, Martin, et al. "
Pembrolizumab
versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer." New England Journal of Medicine (2016).Slide43
Pembrolizumab
group showed better ORR and longer duration of response
KEYNOTE-024
Reck
, Martin, et al. "
Pembrolizumab
versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer." New England Journal of Medicine (2016).Slide44
Treatment-related AE of any grade were less frequent
KEYNOTE-024
Reck
, Martin, et al. "
Pembrolizumab
versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer." New England Journal of Medicine (2016).Slide45
There were no grade 5 immunemediated
events.
KEYNOTE-024
Reck
, Martin, et al. "
Pembrolizumab
versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer." New England Journal of Medicine (2016).Slide46
Hence…October 2016
Based on these results, an independent
Data Monitoring
Committee (DMC) has recommended that the trial be stopped, and that
patients receiving
chemotherapy in KEYNOTE-024 be offered the opportunity to receive
pembrolizumab
.Slide47
Pembrolizumab
+ CT as First-line Therapy for Advanced Nonsquamous NSCLCRandomized phase II cohort of open-label multicohort trial
Primary endpoint: ORR (RECIST v1.1) Secondary endpoints included: PFS, DoR, OS, and safety
Langer CJ, et al. Lancet Oncol. 2016;17:1497-1508.
KEYNOTE-021
(NSCLC – First line)Slide48
First-line CT ±
Pembrolizumab
Langer CJ, et al. Lancet Oncol. 2016;17:1497-1508.
KEYNOTE-021Slide49
Better PFS compared to CT alone.
Langer CJ, et al. Lancet Oncol. 2016;17:1497-1508.
KEYNOTE-021Slide50
OS
0
6
14
25
37
51
57
69
86
113
135
0
Nivolumab
Pts at Risk, n
0
3
7
11
17
22
33
46
69
104
137
Docetaxel
1
Docetaxel
18-mo OS rate: 13%
OS (%)
Mos
Nivolumab
18-mo OS rate: 28%
100
90
80
70
60
50
40
30
10
0
20
33
27
24
21
18
15
12
9
6
3
0
30
12-mo OS rate: 42%
12-mo OS rate: 24%
Reckamp
K, et al. WCLC 2015. ORAL02.01.
Nivolumab (n = 135)
Docetaxel (n = 137)
HR: 0.62 (95% CI: 0.48-0.81;
P
= .0004)
Median OS,
Mos (95% CI)
9.2 (7.33-12.62)
6.0 (5.29-7.39)
Events,
n
103
122
CheckMate
017
Minimum follow-up for survival: 18 mos
International, prospective, randomised, phase 3 trialSlide51
PFS significantly longer with
nivolumab vs docetaxel
Brahmer J, et al. N Engl J Med. 2015;373:123-135.
0
3
6
9
12
15
18
21
24
100
80
60
40
20
0
PFS
(% of Patients)
Mos
Nivolumab
(N = 135)
Docetaxel (N = 137)
HR: 0.62 (95% CI: 0.47-0.81)
P
< .001
Median PFSS,
mo (95% CI)
3.5 (2.1-4.9)
2.8 (2.1-3.5)
1-Yr PFS,
% of pts (95% CI)
21 (14-28)
6 (3-12)
No. of
Events
105
122
CheckMate
017Slide52
ORR favored nivolumab vs docetaxel
(19% vs 12%; P = 0.02)
Nivolumab
Docetaxel
0
16
32
48
64
80
96
112
14% (5 of 36 pts) with ongoing response
52% (29 of 56 pts) with ongoing response
Time to first response
During
nivolumab
treatment
During docetaxel treatment
After discontinuation of treatment
Ongoing response
Wks
CheckMate
057
Borghaei H, et al. N Engl J Med. 2015;373:1627-1639.Slide53
Effect on OS in Predefined Subgroups
0
Nivolumab
Docetaxel
1
2
All randomized pts (NIvo, n = 292; Doc, n = 290). HR was not computed for other subsets with fewer than 10 pts per treatment group.
Borghaei H, et al. N Engl J Med. 2015;373:1627-1639.
Unstratified HR (95% CI)
0.75 (0.62-0.91)
0.81 (0.62-1.04)
0.63 (0.45-0.89)
0.90 (0.43-1.87)
0.73 (0.56-0.96)
0.78 (0.58-1.04)
0.64 (0.44-0.93)
0.80 (0.63-1.00)
0.70 (0.56-0.86)
1.02 (0.64-1.61)
1.18 (0.69-2.00)
0.66 (0.51-0.86)
0.74 (0.51-1.06)
N
582
339
200
43
319
263
179
402
458
118
82
340
160
Subgroup
Overall
Age categorization (yrs)
< 65
≥ 65 and < 75
≥ 75
Sex
Male
Female
Baseline ECOG PS
0
1
Smoking status
Current/former smoker
Never smoked
EGFR
mutation status
Positive
Not detected
Not reported
CheckMate
057 Slide54
Differences Between Approved Agents
Requirement for PD-L1 expression: only pembrolizumabPredictive nature of PD-L1 assay: pembrolizumab is most well validated; nivolumab has a similar assayFirst-line approval: only pembrolizumab alone (if ≥ 50% PD-L1 expression) or in combination with carboplatin/pemetrexed for nonsquamous histology
Schedule: atezolizumab and pembrolizumab every 3 wks vs nivolumab every 2 wks Price: all high; actual cost not entirely transparentSlide55
Future of immuno-oncologySlide56
Recent Early Phase Trials in NSCLC
Agent
Population
Efficacy
Tolerability
Durvalumab
(Anti-PD-L1)
[1]
Squamous
(n = 88)
Nonsquamous
(n = 112)
ORR: 16%
27% in PD-L1+
5% in PD-L1-
Squamous: 21%
Nonsquamous:
13%
Tx-related AEs:
Any: 50% of pts
Grade 3/4: 8%
Leading to d/c: 5%
No
tx
-related colitis or hyperglycemia, no grade 3/4 pneumonitis
Durvalumab
+ tremelimumab (Anti-CTLA-4)[2]
Advanced
NSCLC (n = 102)
ORR: 27%33% PD-L1+ 27% PD-L1-
Tx-related AEs:
Any: 63%-89% of pts by cohortGrade 3/4: 29%-78% by cohortLeading to d/c: 7%-44% by cohortGrade 3/4 immune-related AEs: colitis (9%), pneumonitis (4%), and hypothyroidism (1%) Pembrolizumab + ipilimumab(KEYNOTE-021)[3]Recurrent NSCLC after ≤ 2 regimens (n = 18)ORR: 39%Tx-related AEs: Any: 83% of pts
Grade 3/4: 17% (adrenal insufficiency, maculopapular rash, drug eruption)Leading to d/c: 11%1. Rizvi NA, et al. ASCO 2015. Abstract 8032. 2. Antonia SJ, et al. ASCO 2015. Abstract 3014. 3. Patnaik A, et al. ASCO 2015. Abstract 8011. Slide57
Phase III Trials of New Immune Checkpoint Inhibitors in Advanced NSCLC
1. ClincalTrials.gov. NCT02008227. 2. ClincalTrials.gov. NCT02409342.
3. ClincalTrials.gov. NCT02409355. 4. ClincalTrials.gov. NCT02395172.
5. ClincalTrials.gov. NCT02576574. 6. ClincalTrials.gov. NCT02352948.
Trial
Est. N
Setting
Treatment Arms
Primary
Endpoint
OAK
[1]
1225
Second
line
Atezolizumab vs
docetaxel
OS
IMpower 110
[
2]
400
First
line
Non-SQ
Atezolizumab vs
cisplatin
or carboplatin + pemetrexed
PFS
IMpower 111
[3]
400
First
line
SQ
Atezolizumab vs
cisplatin or carboplatin + gemcitabinePFSJAVELIN Lung 200[4]
650Second lineAvelumab vs docetaxel
OS
JAVELIN Lung 100[5]
420
First
line
Avelumab vs platinum-containing chemotherapy
PFS
ARCTIC
[6]
730
Third line
Durvalumab ±
tremelimumab vs SOC
platinum-based chemotherapy
OS, PFSSlide58
Combination Immunotherapy ??
Sharma P, et al. Science. 2015;348:56-61.Slide59
Phase III First-line Combination Trials in Advanced NSCLC (All PD-L1 Unselected)
1. ClincalTrials.gov. NCT02477826. 2. ClincalTrials.gov. NCT02578680. 3. ClincalTrials.gov. NCT02775435. 4. ClincalTrials.gov. NCT02453282. 5. ClincalTrials.gov. NCT02542293. 6. ClincalTrials.gov. NCT02367781. 7. ClincalTrials.gov. NCT02366143. 8. ClincalTrials.gov. NCT02367794.
Trial
Estimated N
Treatment Arms
Primary Endpoint
Checkmate 227
[1]
1980
Nivo ± ipilimumab, platinum
-based
chemo
OS, PFS
KEYNOTE-189
[2]
570
Pemetrexed/cisplatin ±
pembro
PFS
KEYNOTE-407
[3]
560
Platinum
-based
chemo ±
pembro
OS, PFS
MYSTIC
[4]
675
Durvalumab ±
t
remelimumab,
SOC
platinum
-based chemotherapy
PFS
NEPTUNE[5]800
Durvalumab + tremelimumab,SOC platinum-based chemotherapyOSIMpower 130[6]
550
Nab-paclitaxel/carboplatin ± atezolizumab
PFS
IMpower
150[7]
1200
Paclitaxel/carboplatin +
bevacizumab AND/OR atezolizumab
PFS
IMpower
131[8]
1200
Nab-paclitaxel/carboplatin ± atezolizumab,
paclitaxel/carboplatin + atezolizumab
PFSSlide60
Immune Checkpoint Therapy: What Is Next?
Anti–PD-1/PD-L1
Your favorite treatment
The future of cancer therapySlide61
Management of Cancer in the Post Anti–PD-1/PD-L1 Era
Anti–PD-1/anti–PD-L1
Generate T cells:
+ Anti–CTLA-4
+ Immune-activating antibodies or cytokines
+ TLR agonists or oncolytic viruses
+ IDO or macrophage inhibitors
+ Targeted therapies
Bring T cells into tumors:
Vaccines
TCR-engineered ACT
CAR-engineered ACT
TLR, toll-like receptor; IDO,
indoleamine
-pyrrole 2,3-dioxygenase; CAR, chimeric antigen receptor; ACT, adoptive cell transfer.Slide62
A Roadmap of Immunotherapy-Tumour
Interactions
Chen DS, et al. Immunity. 2013;39:1-10.
4
Trafficking of T cells to tumors
5
Infiltration of T cells into tumors
Anti-VEGF
6
Recognition of cancer cells by T cells
CARs
7
Killing of cancer cells
Anti–PD-L1
Anti–PD-1
IDO inhibitors
1
Release of cancer cell antigens
Chemotherapy
Radiation therapy
Targeted therapy
2
Cancer antigen presentation
Vaccines
IFN-
α
GM-CSF
Anti-CD40 (agonist)
TLR agonists
3
Priming and activation
Anti-CTLA4
Anti-CD137 (agonist)
Anti-OX40 (agonist)
Anti-CD27 (agonist)
IL-2
IL-12Slide63
Take home messageSlide64
Lesson 1: Histology Does Not Help Select Pts for Immunotherapy
1. Brahmer J, et al. N Engl J Med. 2015;373:123-135.
2. Borghaei H, et al. N Engl J Med. 2015;373:1627-1639.
3. Herbst RS, et al. Lancet. 2016;387:1540-1550.
4. Vansteenkiste, et al. ESMO 2015. 14LBA.
5. Fehrenbacher L, et al.
Lancet. 2016;387:1837-1846.Slide65
Lesson 1: Histology Does Not Help Select Pts for Immunotherapy
1. Brahmer J, et al. ASCO 2014. Abstract 8112.
2. Herbst RS, et al. Nature. 2014;515:563-567. Slide66
Lesson 2: Response Is Rapid
Soria JC, et al. ECC 2015. Abstract 33LBA.Slide67
Which Pts Do We Avoid?
Exclusion criteria in previous studies:Performance status ≥ 2Autoimmune diseaseHepatitis, HIVPD-L1 negativeInterstitial lung disease
On “higher dose” steroidsSlide68
Summary
Immune checkpoint inhibitors are a new standard of care for patients with advanced NSCLC who have progressed after platinum-based chemotherapyAssessing PD-L1 expression can provide information on potential efficacy for certain patient subsetsOngoing clinical trials with additional immune checkpoint inhibitors and new combination approaches may expand the utility of these agents in clinical practiceSlide69
Boosting the Potential for Immune Response With Combination Therapies
Modified from Ribas A, et al. Clin Cancer Res. 2012;18:336-341. Slide70
Treatment Algorithm for Advanced NSCLC: Molecular Biomarker PositiveSlide71
Treatment Algorithm for Advanced NSCLC: No Actionable BiomarkerSlide72
Thank you!