
Understand sexual abuse epidemiologybrDistinguish normal sexual behavior from behavior suggestive of abusebrUnderstand the process of reporting and child advocacy center CAC evaluationbrBecome familiar with the medical evaluation including the significance of medical findings ID: 776753
Download Presentation The PPT/PDF document "IDENTIFICATION AND EVALUATION OF SUSPECT..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
IDENTIFICATION AND EVALUATION OF SUSPECTED SEXUAL ABUSE
The District of Columbia Family Court
9
th
Annual Multidisciplinary Training Institute
Wendy
Gwirtzman
Lane, MD, MPH
Katherine
Deye
, MD
Slide2Objectives
Understand sexual abuse epidemiology
Distinguish normal sexual behavior from behavior suggestive of abuse
Understand the process of reporting and child advocacy center (CAC) evaluation
Become familiar with the medical evaluation, including the significance of medical findings
Slide3Case Presentation
You are appointed as Guardian ad Litem for 4 year-old Sara, because of possible parental neglect
Sara’s parents are no longer together. She lives with her mother, mother’s boyfriend, 2 sisters, ages 3 & 7, aunt, and 2 male cousins, ages 12 & 13
Sara sees dad infrequently. Paternal grandmother babysits twice a week
Slide4Case Presentation
You visit Sara for the first time. She is chatty and energetic when alone with you, but quiet when in the presence of her aunt and cousins.
While alone with her, Sara asks you, “Want to see me dance?” and proceeded to perform a very provocative dance.
Slide5Case Presentation
Sara’s mother is angry that CPS is involved with the family and is not very open with you.
While talking with mom, you observe Sara watching TV alone in the next room. She is sitting quietly, rubbing her vaginal area.
Slide6Case Presentation
You meet with Sara’s paternal grandmother the next day. She tells you that Sara always “looks red down there” and “her hole is too open.”
She expresses concern that mom’s boyfriend is abusing Sara.
Slide7Is Sara being sexually abused??What is sexual abuse??
Slide8Definition – CAPTA
“The employment, use, persuasion, inducement, enticement, or coercion of any child to engage in, or assist any other person to engage in, any sexually explicit conduct or simulation of such conduct for the purpose of producing a visual depiction of such conduct; or the rape, and in cases of caretaker or interfamilial relationships, statutory rape, molestation, prostitution, or other form of sexual exploitation of children, or incest with children.”
Slide9Definition
All sexual contact or conduct that is:
Unwanted by a child, or
Manipulative, exploitative, or
Outside developmentally appropriate play
By a parent, caregiver, household, or family member
Neither definition requires injury
Slide10Common Myths
Perpetrators are strangers in trench coats
Children always lie about abuse
Children never lie about abuse
Sexual abuse doesn’t occur in “nice” families
Slide11Historical Context
Late 1900’s – Freud initially tries to expose the problem. Later recants and attributes disclosures to child desires and fantasies.
Late 1960’s – Initial professional acceptance of existence of child maltreatment – Focus on physical abuse, “battered child syndrome”
Slide12Historical Context – 1970’s
1973 – 1
st
article on CSA listed in Index Medicus
1975 - Sgroi calls CSA “the last frontier in child abuse.” Tells physicians “in order to make the diagnosis of CSA, one must entertain the possibility that it occurs.”
Slide13Historical Context – 1980-on
1980’s -Increased acceptance of CSA by professionals & establishment of CAC’s
Late 80’s backlash against diagnosis
1990’s & beyond- gradual increase in knowledge, improvements in practice
Slide14Epidemiology
Reported cases are the tip of the iceberg
Level 1
Known to CPS
Level 2
Known to Other
Investigatory Agencies
Level 3
Known to Professionals in schools,
hospitals, and other major agencies
Level 4
Known to other agencies and individuals
Level 5
Known to no one
Slide15Known cases are just the tip of the iceberg
Slide16Epidemiology
PREVALENCE
19% of women
9% of men
abused as children
Slide17Perpetrator Characteristics
No typical profile
Many appear normal, successful & have no criminal record
Most are male
Most are familiar to the child many in position of trust, authority
20-40% adolescents
Many (not all) were abused themselves
Slide18Child Characteristics
About 85% female (cases known to system)
Peak ages:
Girls and boys – early school age 5-7 years
Girls – 14-15 years
Vulnerable, needy
Slide19Longitudinal Progression of Abuse (Sgroi, 1982)
Engagement – development of relationship
Sexual Interaction – progressive
Secrecy – bribes, threats
Disclosure – accidental or purposeful
Suppression
Slide20Child Sexual Abuse Accommodation Syndrome
(Summit, 1983)
Secrecy
Helplessness
Entrapment & Accommodation
Unconvincing disclosure
Retraction
Helps explain delayed disclosure
Slide21Impact of Sexual Abuse –
Physical Health
Short term
Acute injuries
STD’s
Long term:
GI problems (irritable bowel)
Chronic pain (headache, abdominal, back, or pelvic pain)
Obesity, failure to thrive
Somatization
Slide22Impact of Sexual Abuse –
Mental Health
Behavioral problems – withdrawal, acting out, delinquency
Depression
PTSD & other anxiety disorders
Substance abuse
Eating disorders – anorexia, bulemia
School failure
Low self esteem, interpersonal difficulties
Slide23Ways Children May Be Identified
Physical signs: injury or infection
Child’s disclosure – to another child, parent, therapist, or trusted adult
Child sexually abuses another child
Child uses sexually explicit language, behavior beyond normal development
Slide24Developmental Considerations
in Disclosure
Ages 0-4
Often can’t give reliable disclosure
Diagnosis by medical evidence, reported symptoms of physical or emotional trauma
Ages 5-7
Give simplistic description of abuse
May see sexual acting out (in play and on others), sleep problems
Slide25Developmental Considerations
in Disclosure
Ages 8-11
Allegations clearer, more specific
Boys may be more reluctant to disclose
Self-blame
Ages 12-16
May see promiscuity, depression, withdrawal, suicide attempts
Physical maturity confused with emotional maturity – girls may not see abuse as such
Slide26Sexualized Behavior in Children
Possible causes:
Sexual abuse
Poor understanding of societal norms
E.g. child with mental retardation
Sexual curiosity/exploration
Exposure to explicit sexual activities
Witnessed activity in home, on TV, movies
Viewing pornography
May be inadvertent, neglectful, or abusive
Slide27Common Behaviors @ 2-9 years
(unlikely to be related to abuse)
Friedrich WN. Normative sexual behavior in chidren. Pediatrics. 1998; 101:e9
Boys
Touches sex parts at home
Touches breasts
Stands too close
Tries to look at other people when they are nude
Touches sex parts in public
Masturbates with hand
Girls
Touches sex parts at home
Touches breasts
Tries to look at other people when they are nude
Stands too close
Masturbates with hand
Touches sex parts in public
Slide28Common Behaviors @ 10-12
(unlikely to be related to abuse)
Friedrich WN. Normative sexual behavior in chidren. Pediatrics. 1998; 101:e9
Boys
Very interested in opposite sex
Wants to watch TV nudity
Tries to look at pictures of nude people
Knows more about sex
Talks about sex acts
Touches sex parts at home
Girls
Very interested in opposite sex
Knows more about sex
Stands too close
Wants to watch TV nudity
Touches sex parts at home
Talks about sex acts
Slide29Uncommon Behaviors @ 2-12
(more likely to be related to abuse)
Puts mouth on sex parts
Asks to engage in sex acts
Masturbates with object
Inserts objects in vagina/anus
5) Imitates intercourse
Makes sexual sounds
Tries to french kiss
Undresses other people
Asks to watch explicit TV
10) Imitates sexual behavior with dolls
Slide30Behaviors that Raise Concern
Excessive focus on sexuality, knowledge beyond normal development
Inappropriate behavior despite redirection
Sexual behavior/exploration/coercion with much older/younger children
Inflicts injury to own or other’s genitals
Disturbing toileting behavior
Drawings with genitals predominating
Sexual contact with animals
Slide31What to do if you observe…
Calm, non-judgemental questioning
“Where did you learn about that/how to do that?”
Don’t push child to answer
Slide32Back to Sara…
Based on your observations and interviews, you decide to:
Do nothing
Report to CPS
Report to Police
Provide information to grandmother about reporting
B and C
Slide33Back to Sara…
Grandmother decides to call CPS to report suspected sexual abuse
The report is accepted for investigation
Grandmother wants to take Sara to the local emergency department, “so the doctor can tell me if she’s been touched”
Slide34What do You Tell Grandma?
Immediate medical exam only necessary if:
Abuse occurred in past 72-96 hours
Child is having serious physical or psychological symptoms
Immediate exam generally needed to:
Document injury
Collect forensic evidence (saliva, blood, semen)
Exam should only be done by clinician trained to do sexual abuse evaluations!!!!
Slide35What Happens Next??
You successfully dissuade Grandma from bringing Sara to the ED.
The next day, an investigator from CPS contacts Sara’s mother.
She schedules an interview at the local child advocacy center
Slide36The Child Advocacy Center
Sara’s mother wants to know what is going to happen at her appointment
What do you tell her?
Slide37What Happens at the CAC?
Forensic interview
Sara is interviewed by trained professional.
May be CPS worker, other social worker, or psychologist
Interview may be taped, observed by camera or 1-way mirror
Medical evaluation (in 2011)
By physician or nurse with special training in child sexual abuse
Slide38Safe Shores (CAC in DC)
Bundy School
Art Therapy Room
Slide39Safe Shores/CNMC Medical Suite
Medical Suite &
Colposcope
Slide40Why does she need a specialist??
Little training in medical school & residency about examination of female anatomy
Many practitioners don’t routinely examine children’s genitals – not familiar with what’s normal & abnormal
Expert often has camera/colposcope to improve visualization, document findings
Slide41The Medical Evaluation
Interview with parent
Explain process
Possible questions about reason for visit
Obtain medical history
Elicit signs/symptoms that may indicate abuse
Interview with child
Explain exam in simple way “nose to toes check-up”, nothing that will hurt
Slide42Examination Techniques
Frog Leg Position
Supine Knee Chest Position
Slide43Myths About the Exam
The doctor can tell for sure if she’s been abused
The doctor can tell if she’s been penetrated
The doctor needs to look inside of her
If she has a hole in her hymen, she’s been abused
If the hole is too big, she’s been abused
Slide44The Medical Evaluation - Findings
“It’s normal to be normal”
More than 95% of referred children have normal exams
Why???
Abusive acts may leave no injury (e.g. fondling)
Causing injury increases risk of disclosure
Injuries often heal without scars before disclosure and medical evaluation
Slide45The Medical Evaluation – What’s Not Normal
Genital injury –
Acute - tears, bruises, bite marks
Sub-acute, chronic – healed hymenal tears, scars
Sexually transmitted diseases
Pregnancy
Forensic evidence – sperm, semen, etc.
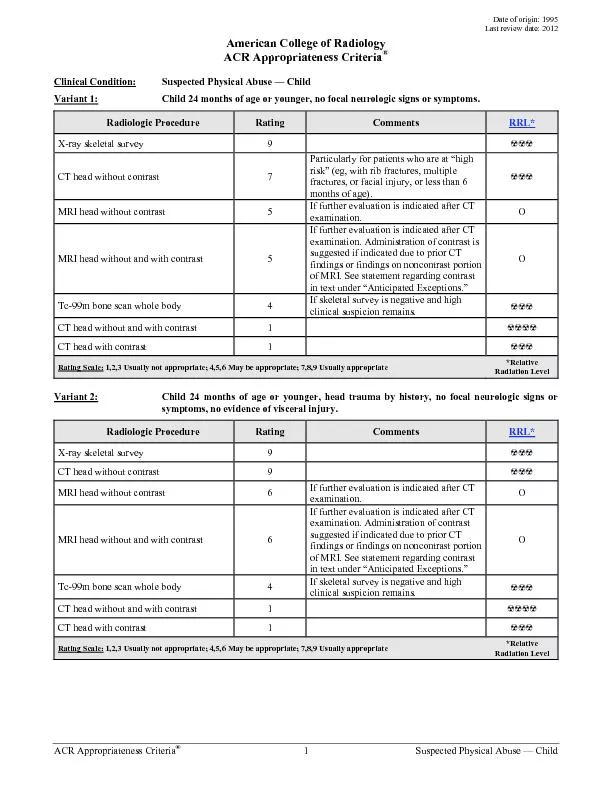
Slide46Implications of Commonly Encountered STDs
STD Confirmed
Sexual Abuse
Suggested Action
Gonorrhea*
Diagnostic
Report
Syphilis*
Diagnostic
Report
HIV infection
Diagnostic
Report
C.
trachomatis
infection*
Diagnostic
Report
T.
vaginalis
infection
Highly suspicious
Report
HPV (
anogential
warts)
Suspicious
Report
Herpes simplex (genital location)
Suspicious
Report
Bacterial
vaginiosis
Inconclusive
Medical follow-up
*If not perinatally acquired and rare nonsexual transmission is
excluded
Adapted from Kellogg, N; AAP, Committee on Child Abuse & Neglect. Pediatrics. 2005; 116(2): 506-512
Slide47Sexually Transmitted Diseases
In infants & toddlers, need to consider possibility of transmission from mother during pregnancy, birth.
In adolescents, need to consider transmission via consensual sex
Diagnosis of gonorrhea, chlamydia, or syphilis make sexual abuse highly likely
Slide48If the doctor can’t give me an answer, why have an exam???
Document injuries, if present
Test for infection
PROVIDE REASSURANCE –
“Everything looks normal and healthy”
Slide49What is done with the information from the medical exam???
Findings provided to CPS worker, police.
Determination made based on combination of medical findings, child interview, and other available data
Substantiated – abuse occurred
Unsubstantiated – abuse may have occurred
Ruled-out – abuse did not occur
Slide50Questions???