
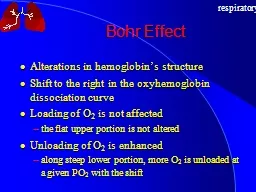
RESPIRATORY CARE MAY 2013 VOL 58 NO 5 Paul F Nuccio MS RRT FAARC Brigham and Womens Hospital Boston MA Background Definitions PSV Pressure Support Ventilation NAVA Neurally ID: 816210
Download The PPT/PDF document "Effect of Ventilatory Variability on Occ..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Effect of Ventilatory Variability on Occurrence of Central ApneasRESPIRATORY CARE • MAY 2013 VOL 58 NO 5
Paul F. Nuccio, MS, RRT, FAARC
Brigham and Women’s Hospital
Boston, MA
Slide2BackgroundDefinitions:
PSV = Pressure Support Ventilation
NAVA =
Neurally
Adjusted Ventilatory Assist
Periodic breathing
What is the research question?
Is there a difference in the occurrence of central apnea episodes between patients ventilated with a constant-level PSV vs. NAVA?
Is this research question relevant?
Central apnea may be associated with significant
pathophysiologic
changes, including stroke, brainstem lesion, encephalitis, and congestive heart failure.
Slide3BackgroundWhat is known about this subject?
normal ventilation varies from breath to breath
traditional mechanical ventilation may be monotonous
close association between arousal from sleep and ventilatory effort
Background literature
Anesthesiology 2010;112(3):670-681.
NAVA resulted in more complexity of airflow and breathing pattern compared with PPV
Anesthesiology 2009;110(2):342-350.
Variability of pressure support improves lung function
Any concerns about COI?
None. Dr.
Delisle
has disclosed a relationship with Fisher &
Paykel
.
Slide4Methods
What is the study design?
Prospective, comparative, crossover study
Inclusion criteria
Invasive mechanical ventilation
Normal consciousness
Absence of sedatives and opiates for
>
24 hours
PSV with FiO2 <0.60 and PEEP of 5cmH2O (SpO2
>
90%)
Exclusion criteria
Presence of a central nervous system disorder
Glasgow Coma Scale score <11
Hemodynamic instability
Renal and/or hepatic insufficiency
Ongoing sepsis
History of esophageal
varices
or
gastroesophageal
bleeding (past 30 days)
History of GI symptoms such as vomiting
Slide5Methods
What is the control group?
With a crossover study, every patient serves as his or her own control.
Is the sample size appropriate?
There were a total of 14 patients in the study.
Very difficult to draw conclusions from such a small sample size.
What are the threats to validity of the design?
Small sample size
Compare apples to apples?
Was the statistical analysis appropriate?
Statistical software utilized for analysis
Comparisons made using general linear model for repeated measures
Wilcoxon
test for paired samples
Any ethical concerns?
The ethics committee of the hospital approved the study, and the subjects or their surrogates gave their informed consent.
Potential ethics concerns if one therapy appears to provide more benefit.
Slide6Study
Protocol
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide7Polysomnography
tracings with
neurally
adjusted ventilatory assist (NAVA) and pressure support ventilation (PSV) in a representative subject.
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide8ResultsWhat are the main results? Study population
See table 1
Breathing pattern
See table 2
Apneas
See table 3
Variability of ventilation
See table 4
Slide9Table 1 - Subjects
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide10Table 2 - VT
, Breathing Frequency,
Apneas
per Hour, and PETCO2 While
Awake
and Asleep.
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide11Table 3 - Oscillatory
Behavior
of VT, Breathing Frequency, V̇E, and PETCO2 During Sleep Stages 2 and 3–4 During PSV in the 10 Patients With Central
Apneas
.
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide12Table 4 - VT
, f-flow, and
EAdi
Peak Variability in the 10 Patients With
Central
Apneas
.
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide13Fig 3 - Variability
during pressure support ventilation (PSV).
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide14Fig 4 - Variability
during
neurally
adjusted ventilatory assist (NAVA).
Delisle
, S. et al.
Respir
Care 2013;58:745-753
(c) 2012 by
Daedalus
Enterprises, Inc.
Slide15DiscussionWhat do these finding mean?
Interesting & provocative study that lacks clear clinical outcomes benefit
How should these findings impact practice?
Unlikely to have a significant impact on practice
How do these findings relate to previous findings from other studies?
Similar to other studies
Slide16DiscussionWhat are the study limitations/concerns?
Single center study
Small sample size
Possible influence of sedation
Single level of both NAVA and PSV
Potential risk of using NG tubes
What additional work is needed in this area?
Study findings of physiological effect of NAVA must be confirmed by further clinical studies.
Slide17Editorial… by Kathy S Myers Moss MEd RRT-ACCS University of Missouri
“I commend the authors on their use of a prospective, randomized, controlled trial, the gold standard of experimental research methods. In addition, the research design integrated a crossover method with attention to minimizing residual effects. The statistically significant effect on tidal volume variation is especially noteworthy given the small sample size of 14.’’
“Until well designed studies provide evidence suggesting reduced morbidity, mortality, stay, number of ventilator days, or other desirable clinical outcomes, clinical managers are unlikely to invest in the required software and hardware upgrades necessary to implement NAVA.”
Slide18ConclusionsWhat are the authors’ conclusions?NAVA was associated with increased ventilatory variability compared to constant level PSV. With NAVA absence of
overassistance
during sleep coincided with absence of central apneas, suggesting that load capacity and/or
neuromechanical
coupling were improved by NAVA and that this improvement decreased or abolished central apneas.
How do you think this should affect practice?
Since NAVA is exclusively an option for one ventilator, widespread use of this technology will continue to be limited. More widespread adoption of this technology will require physiologic outcomes improvements, outcomes such as decreased number of ventilator days, and fewer complications of mechanical ventilation.
What is the take-home message?
Further clinical investigations are needed to evaluate the impact of NAVA on weaning time and patient outcomes.