
2 MSPH Ashok K Hemal 1 MD Ram A Pathak 1 MD 1 Department of Urology Wake Forest School of Medicine WinstonSalem NC 2 Division of Public Health Sciences Wake Forest School of Medicine WinstonSalem NC ID: 1040702
Download Presentation The PPT/PDF document "Vanessa A. Lukas 1 , MS4; Tim Craven" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




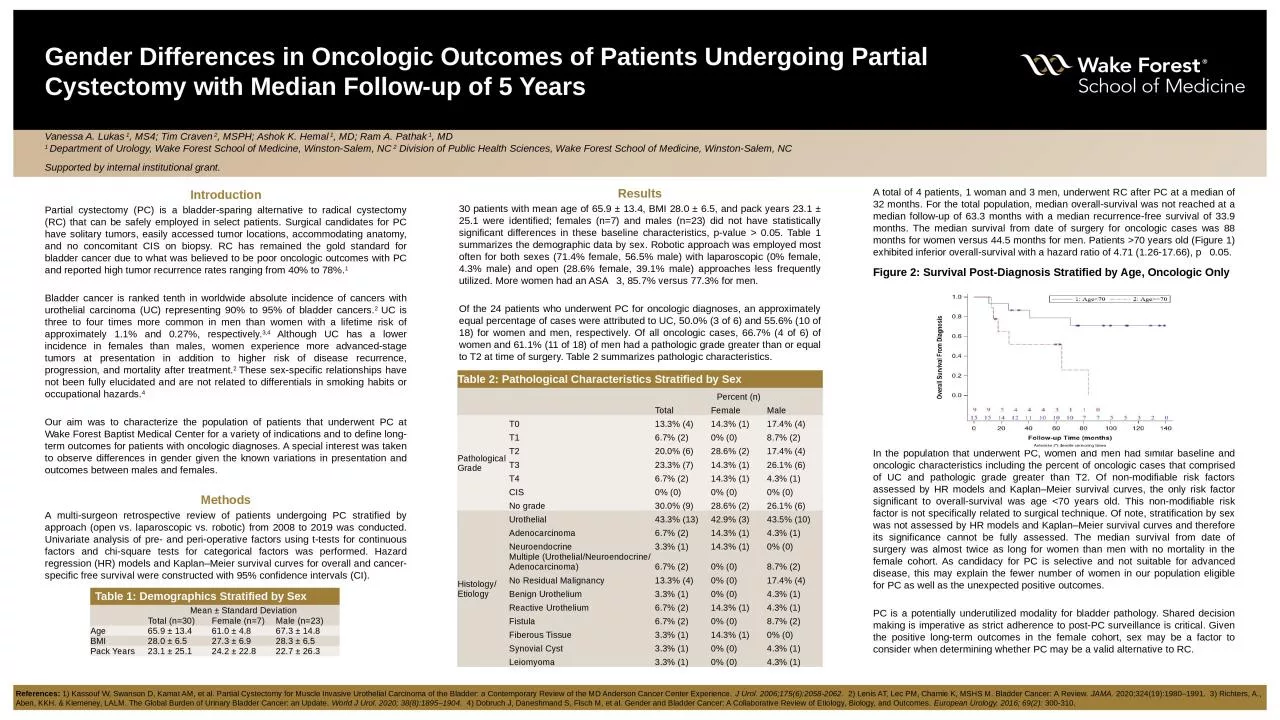
1. Vanessa A. Lukas 1, MS4; Tim Craven 2, MSPH; Ashok K. Hemal 1, MD; Ram A. Pathak 1, MD1 Department of Urology, Wake Forest School of Medicine, Winston-Salem, NC 2 Division of Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, NC Supported by internal institutional grant.Gender Differences in Oncologic Outcomes of Patients Undergoing Partial Cystectomy with Median Follow-up of 5 YearsIntroductionPartial cystectomy (PC) is a bladder-sparing alternative to radical cystectomy (RC) that can be safely employed in select patients. Surgical candidates for PC have solitary tumors, easily accessed tumor locations, accommodating anatomy, and no concomitant CIS on biopsy. RC has remained the gold standard for bladder cancer due to what was believed to be poor oncologic outcomes with PC and reported high tumor recurrence rates ranging from 40% to 78%.1Bladder cancer is ranked tenth in worldwide absolute incidence of cancers with urothelial carcinoma (UC) representing 90% to 95% of bladder cancers.2 UC is three to four times more common in men than women with a lifetime risk of approximately 1.1% and 0.27%, respectively.3,4 Although UC has a lower incidence in females than males, women experience more advanced-stage tumors at presentation in addition to higher risk of disease recurrence, progression, and mortality after treatment.2 These sex-specific relationships have not been fully elucidated and are not related to differentials in smoking habits or occupational hazards.4Our aim was to characterize the population of patients that underwent PC at Wake Forest Baptist Medical Center for a variety of indications and to define long-term outcomes for patients with oncologic diagnoses. A special interest was taken to observe differences in gender given the known variations in presentation and outcomes between males and females.MethodsA multi-surgeon retrospective review of patients undergoing PC stratified by approach (open vs. laparoscopic vs. robotic) from 2008 to 2019 was conducted. Univariate analysis of pre- and peri-operative factors using t-tests for continuous factors and chi-square tests for categorical factors was performed. Hazard regression (HR) models and Kaplan–Meier survival curves for overall and cancer-specific free survival were constructed with 95% confidence intervals (CI). Results30 patients with mean age of 65.9 ± 13.4, BMI 28.0 ± 6.5, and pack years 23.1 ± 25.1 were identified; females (n=7) and males (n=23) did not have statistically significant differences in these baseline characteristics, p-value > 0.05. Table 1 summarizes the demographic data by sex. Robotic approach was employed most often for both sexes (71.4% female, 56.5% male) with laparoscopic (0% female, 4.3% male) and open (28.6% female, 39.1% male) approaches less frequently utilized. More women had an ASA 3, 85.7% versus 77.3% for men.Of the 24 patients who underwent PC for oncologic diagnoses, an approximately equal percentage of cases were attributed to UC, 50.0% (3 of 6) and 55.6% (10 of 18) for women and men, respectively. Of all oncologic cases, 66.7% (4 of 6) of women and 61.1% (11 of 18) of men had a pathologic grade greater than or equal to T2 at time of surgery. Table 2 summarizes pathologic characteristics.A total of 4 patients, 1 woman and 3 men, underwent RC after PC at a median of 32 months. For the total population, median overall-survival was not reached at a median follow-up of 63.3 months with a median recurrence-free survival of 33.9 months. The median survival from date of surgery for oncologic cases was 88 months for women versus 44.5 months for men. Patients >70 years old (Figure 1) exhibited inferior overall-survival with a hazard ratio of 4.71 (1.26-17.66), p 0.05. Figure 2: Survival Post-Diagnosis Stratified by Age, Oncologic Only ConclusionsIn the population that underwent PC, women and men had similar baseline and oncologic characteristics including the percent of oncologic cases that comprised of UC and pathologic grade greater than T2. Of non-modifiable risk factors assessed by HR models and Kaplan–Meier survival curves, the only risk factor significant to overall-survival was age <70 years old. This non-modifiable risk factor is not specifically related to surgical technique. Of note, stratification by sex was not assessed by HR models and Kaplan–Meier survival curves and therefore its significance cannot be fully assessed. The median survival from date of surgery was almost twice as long for women than men with no mortality in the female cohort. As candidacy for PC is selective and not suitable for advanced disease, this may explain the fewer number of women in our population eligible for PC as well as the unexpected positive outcomes.PC is a potentially underutilized modality for bladder pathology. Shared decision making is imperative as strict adherence to post-PC surveillance is critical. Given the positive long-term outcomes in the female cohort, sex may be a factor to consider when determining whether PC may be a valid alternative to RC.Table 1: Demographics Stratified by SexMean ± Standard DeviationTotal (n=30)Female (n=7)Male (n=23)Age65.9 ± 13.461.0 ± 4.867.3 ± 14.8BMI28.0 ± 6.527.3 ± 6.928.3 ± 6.5Pack Years23.1 ± 25.124.2 ± 22.822.7 ± 26.3Table 2: Pathological Characteristics Stratified by SexPercent (n)TotalFemaleMalePathological GradeT013.3% (4)14.3% (1)17.4% (4)T16.7% (2) 0% (0)8.7% (2)T220.0% (6)28.6% (2)17.4% (4)T323.3% (7)14.3% (1)26.1% (6)T46.7% (2)14.3% (1)4.3% (1)CIS0% (0)0% (0)0% (0)No grade30.0% (9)28.6% (2)26.1% (6)Histology/EtiologyUrothelial43.3% (13)42.9% (3)43.5% (10)Adenocarcinoma6.7% (2)14.3% (1)4.3% (1)Neuroendocrine3.3% (1)14.3% (1)0% (0)Multiple (Urothelial/Neuroendocrine/Adenocarcinoma)6.7% (2)0% (0)8.7% (2)No Residual Malignancy13.3% (4)0% (0)17.4% (4)Benign Urothelium3.3% (1)0% (0)4.3% (1)Reactive Urothelium6.7% (2)14.3% (1)4.3% (1)Fistula6.7% (2)0% (0)8.7% (2)Fiberous Tissue3.3% (1)14.3% (1)0% (0)Synovial Cyst3.3% (1)0% (0)4.3% (1)Leiomyoma3.3% (1)0% (0)4.3% (1)References: 1) Kassouf W, Swanson D, Kamat AM, et al. Partial Cystectomy for Muscle Invasive Urothelial Carcinoma of the Bladder: a Contemporary Review of the MD Anderson Cancer Center Experience. J Urol. 2006;175(6):2058-2062. 2) Lenis AT, Lec PM, Chamie K, MSHS M. Bladder Cancer: A Review. JAMA. 2020;324(19):1980–1991. 3) Richters, A., Aben, KKH. & Kiemeney, LALM. The Global Burden of Urinary Bladder Cancer: an Update. World J Urol. 2020; 38(8):1895–1904. 4) Dobruch J, Daneshmand S, Fisch M, et al. Gender and Bladder Cancer: A Collaborative Review of Etiology, Biology, and Outcomes. European Urology. 2016; 69(2): 300-310.