
Martha Cannon BA VetMB DSAMFel RCVS Specialist in Feline Medicine Oxford Cat Clinic Definitions Acute kidney injury AKI sudden damage to an otherwise healthy kidney loss of function spectrum from mild to severe ID: 1031740
Download Presentation The PPT/PDF document "Acute Kidney Disease: Priorities in inv..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




1. Acute Kidney Disease: Priorities in investigation and treatmentMartha Cannon BA VetMB DSAM(Fel) RCVS Specialist in Feline MedicineOxford Cat Clinic
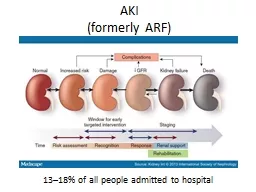
2. DefinitionsAcute kidney injury (AKI): sudden damage to an otherwise healthy kidney+/- loss of function, spectrum from mild to severePermanent damage is not inevitableAcute renal failure (ARF): abrupt deterioration in renal function resulting in azotaemia and associated metabolic changesPotentially reversible conditionFrequently leads to chronic kidney damage = irreversibleAcute on Chronic Kidney Disease: very commonAcute complication or additional AKI to a kidney with pre-existing (often subclinical) CKD
3. AKI: Sudden Damage to an Otherwise Healthy Kidney Toxins:Lily toxicityEthylene glycolNSAIDsRenal Outflow ObstructionUrethral obstructionUreteral obstructionCommon Causes in CatsTraumaInfectionPyelonephritisFIPNeoplasiaIschaemic damageHypotensionRenal infarctsReduced cardiac outputLily pollenRenal Lymphosarcoma
4. Acute Kidney InjuryAcute Kidney Injury damage is reversible if:Cause can be identified promptlyCause is reversiblePrompt aggressive treatment is possibleBut – prognosis is guarded:Reported cases: mortality 47-64%30-50% of survivors have CKDWorwag + Langston J Am Vet Med Assoc 2008; 232: 728–732. Lily pollenRenal Lymphosarcoma
5. Recognising AKINot all cats that suffer an AKI develop azotaemia (ARF)AKI is identified by finding any of the following criteria:Clinical history, laboratory or diagnostic imaging evidence of kidney insultOrOliguria / Anuria = Urine output < 1 ml/kg/hr over 6 hoursOrProgressive increase in creatinine > 26.4 mol/L within 48 hours, even if creatinine remains within the reference rangeOrVolume responsiveness: fluid therapy produces a decrease in creatinine within 48 hours, or return of urine output within 6 hours
6. IRIS – AKI DIAGNOSIS and GRADINGNB: Grade (and subgrade) will change with treatment and/or progression of disease. This is not a stable permanent disease Grade Creatinine1, non-azotaemic < 140mol/L2, mild AKI 141-220mol/L3, moderate AKI 221-439mol/L4, severe AKI 440-880mol/L5, very severe AKI > 880mol/L www.iris-kidney.com/guidelines/gradingFurther subgrades: Non-oliguric (NO) / Oliguric/anuric (O) urine output < 1 ml/kg/hrRequiring renal replacement therapy (RRT)Life threatening iatrogenic or clinical consequences of ARF
7. Oliguria / ANuriaIndicators: Bladder not fillingRapid, marked increase in azotemiaHyperkalemiaHyperphosphatemiaUrine output may return in response to fluid therapyLook for return of urine output within 6 hoursIf not responsive to fluid therapy aloneFrusemide: 2-4 mg/kg i/v, repeat q 1 hour if no responseIf still no responseFatal prognosis unless renal replacement therapy is availableMannitol + Dopamine not recommendedno evidence of benefithigh risk of adverse effects
8. IRIS – AKI DIAGNOSIS and GRADINGPrognosis depends on the cause and the degree to which treatment of the cause is possible. The grade will change with treatment / disease progression, and this will alter the prognosisGrades 1 and 2: Optimistic for return of function within 2-5 days (with appropriate treatment)Grades 3+, or Grade deteriorates despite treatment: May need weeks of supportive treatment if renal repair is to occurGrades 4 + 5: May be fatal despite treatmentOliguria / Anuria:Fatal unless responds rapidly to fluid therapy (or RRT is available)
9. Scraps: 8 y/o MN DSHChronic problems = DJD and IBDCurrent problemPoorly controlled IBD: voracious appetite, weight loss, diarrhoeaSudden onset lethargy and resents handlingPain on palpation of left kidneySize, outline and texture appears normal
10. Right KidneyLeft KidneyLeft Ureter
11. Scraps: 8 y/o MN DSHIRIS Grade Creatinine1, non-azotaemic < 140mol/L2, mild AKI 141-220mol/L3, moderate AKI 221-439mol/L4, severe AKI 440-880mol/L5, very severe AKI > 880mol/LPrognosis?Grades 1 and 2: Optimistic for return of renal function within 2-5 days with appropriate treatmentGrades 3+, or Grade deteriorates despite treatment: May need weeks of supportive treatment if renal repair is to occurGrades 4 + 5: May be fatal despite treatmentProducing large volumes of urine = non-oliguric
12. Scraps: 8 y/o MN DSHSerial creatinine measurementsDoes Scraps have unilateral or bilateral kidney disease?Does Scraps have acute or chronic kidney disease?
13. Scraps: 8 y/o MN DSHUnilateral or bilateral kidney disease?Left ureter obstructed; Right kidney appears normalAzotemia: Creatinine 249 umol/LAzotemia suggests loss of > 75% kidney functionAcute or Chronic?Acute On Chronic = An acute complication or an additional AKI to a kidney with pre-existing (often subclinical) CKD
14. Acute on chronic kidney diseaseVery common presenting problemCat with previously diagnosed CKD, or “not yet diagnosed” CKDAKI because of a complication of CKDinappetence, vomiting, dehydrationUTI / PyelonephritisHypertensive episodeUreteral obstructionAKI for unrelated reasonHit by car, attacked by a dogHeart failureEpisode of pyrexia ➪ inappetence and dehydration
15. Acute on chronic kidney diseaseChronic Kidney Damage is permanent, Acute Kidney Injury is notSudden deterioration in kidney function in a cat with previously stable CKDSeek a cause of AKIThe deterioration may not be permanent and irreversibleRe-assess the level of CKD after treating the AKI
16. Acute on chronic kidney diseaseClinical SignificancePre-existing CKD will remain even if the AKI can be successfully managedAKI may cause further damage, so the CKD gets worseCannot distinguish temporary damage from permanent damage until after the AKI has been treated
17. Scraps: 8 y/o MN DSHAcute on Chronic Kidney DiseaseLeft ureter obstructedRight kidney appears normal, but can’t be functioning normallyAzotemia suggests loss of > 75% kidney functionCreatinine 249 mol/LCannot attribute an IRIS CKD stage due to the concurrent AKIRestore output from left kidney, stabilise the cat, re-assess kidney function after the event
18. Ureteral ObstructionManage AKI and associated clinical signs and metabolic disturbancesMedical management of ureteral obstructionIntravenous fluids to restore euvolemia and encourage urine production+/- anti-spasmodic medications e.g. amitriptyline No proven benefitSurgical management indicated if:No movement of an obstructive ureterolith over 48–72 horAzotaemia and electrolyte disturbances deteriorate despite treatment
19. Ureteral ObstructionDogs: Surgically induced complete unilateral ureteral obstruction in healthy dogs: Vaughan + Gillenwater (1971) J Urol 106: 27–35.7 days obstruction => no permanent damage 14 days obstruction => approx 70% of GFR recovery within 6 months28 days obstruction => 25–30% of function returned> 42 days obstruction => no return of GFRBut:Many clinical cases have pre-existing CKDMajority of clinical cases – date of onset of obstruction not known
20. Ureteral obstructionSurgical ManagementLithotripsy not useful in catsCalcium oxalate stones are very dense, feline ureter is very small. Energy required to break up the ureteroliths exceeds the tolerance of the ureterSurgical placement of stentSurgical placement of subcutaneous ureteric by-pass (SUB)
21. Subcutaneous Ureteric Bypass
22. Scraps:11 y/o MN DSHAlive and well 3 years on
23. IRIS – DIAGNOSIS and GRADINGPrognosisStage 1 and 2Optimistic for return of renal function within 2-5 days with appropriate treatmentStages 3+, or Stage progresses despite treatment:May require weeks of supportive treatment if renal repair is to occurStages 4 + 5: May be fatal despite treatmentGrade 1, non-azotaemic creatinine < 140mol/LGrade 2, mild AKI creatinine 141-220mol/LGrade 3, moderate AKI creatinine 221-439mol/LGrade 4, severe AKI creatinine 440-880mol/LGrade 5, very severe AKI creatinine > 880mol/L Further subgrades: Non-oliguric (NO)Oliguric/anuric (O) = Urine Output < 1 ml/kg/hrRequiring renal replacement therapy(RRT).Oliguria / Anuria:Fatal unless responds rapidly to treatment (or RRT available)
24. Managing Acute kidney injuryTreat the primary cause where possibleFluid TherapyRestore normal hydrationDo not attempt to induce forced diuresisKidneys may not have the capacity to produce increased urine volumeCan rapidly develop generalised oedema ➪ further organ failureManage HyperkalemiaRestore normal hydration and urine outputPotassium > 7.5 mmol/LInsulin (0.2 iu/kg i/v) with i/v glucose supplement for up to 12 hoursContinue until kidneys revert to excreting potassium
25. Managing Acute kidney injuryOther supportive / symptomatic treatment as required:Anti-nausea: maropitant, ondansetron, mirtazapineAnti-acids: omeprazole, famotidineAnalgesia: buprenorphine, methadoneNutritional support: oesophagostomy tube if indicatedAntibiotics: if evidence of bacterial infection
26. DefinitionsAcute kidney injury (AKI): sudden damage to an otherwise healthy kidney+/- loss of function, spectrum from mild to severeAcute renal failure (ARF): abrupt deterioration in renal function resulting in accumulation of uremic toxins and associated metabolic, electrolyte, fluid balance and acid-base abnormalities.Potentially reversible conditionFrequently leads to chronic kidney damage = irreversibleAcute on Chronic Kidney Disease: very commonAcute complication or additional AKI to a kidney with pre-existing, often subclinical CKD
27. Any Questions?