
Lauren Cosolo RN BScN MN Outline Review bone marrow failure and disease Discuss Myelodysplastic syndrome pathophysiology clinical presentation diagnosis treatment Discuss Aplastic Anemia ID: 910717
Download Presentation The PPT/PDF document "Bone Marrow Failure Diseases: Including ..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
Bone Marrow Failure Diseases: Including MDS, AA, PNH
Lauren
Cosolo
, RN, BScN, MN
Slide2Outline
Review bone marrow failure and disease
Discuss
Myelodysplastic
syndrome, pathophysiology, clinical presentation, diagnosis, treatment
Discuss Aplastic Anemia,
clinical presentation, diagnosis,
treatment
Discuss PNH
, pathophysiology, clinical presentation, diagnosis,
treatment
Review nursing considerations for bone marrow failure diseases
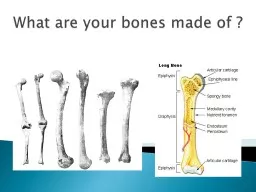
Slide3Bone Marrow Failure
Ineffective hematopoiesis causing pancytopenia and the inability to produce healthy blood cells
Pancytopenia= reduction in blood counts
red cells, white cells, platelets
Image taken from: http://www.lookfordiagnosis.com/mesh_info.php?term=Myeloid+Cells&lang=1
Scheinberg
,
DeZern
,
Steensma
, 2016;
Hoffbrand
& Moss, 2016
Slide4Bone Marrow Failure Diseases
Disorders resulting in
cytopenia
(low blood counts) due to decreased bone marrow production
Can be congenital (inherited) or acquired disorders
Young, 2014; Zhang, 2016
Slide5Myelodysplastic Syndromes (MDS)
Clonal
disorders of hematopoietic stem cells characterized by increasing bone marrow failure in association with dysplastic changes (cells look abnormal) in one or more cell lineages
Simultaneous proliferation and apoptosis of hematopoietic cells (ineffective hematopoiesis) leading to
hypercellular
bone marrow but pancytopenia in peripheral blood
Pathologyoutline.com
Slide6Pathophysiology of MDS
There is an abnormal regulation of proliferation, maturation and survival of hematopoietic stem cells due to genetic changes
A
number of genetic changes/mutations are associated with MDS
Changes in the expression of genes, such as
hypermethylation
contributes to the development or progression of MDSResulting in suppression of gene transcriptionAs the disease progresses, maturation of stem cells are further impaired with increased survival of myeloblasts
Slide7Prevalence and Risk Factors
MDS usually develops in older adults >60 years old with median age of 72-76 years
More common in males than in females
MDS relatively common disease
4-7
estimated new
cases/100,000 each yearRisk Factors: Older ageMaleExposure to environmental factors (benzene)Smoking Previous chemotherapy or radiation treatment
Buckstein & Wells, 2008
Slide8Etiology
Devine, 2013; Aster & Stone, 2018
Slide9Clinical Presentation
Patients with MDS typically present with peripheral blood
cytopenias
Patients range from being asymptomatic with an incidental CBC finding to having symptoms and complications related to the previously unrecognized
cytopenia
Majority of MDS patients present with red cell lineage dysplasia (anemia)
Signs and Symptoms include: Fevers, infection from neutropeniaPetechiae, ecchymosis, bruising, bleeding from thrombocytopeniaFatigue, SOB, palpitations, weakness, exercise intolerance, dizziness, pale complexion, cognitive impairment as result of anemia
Slide10Diagnosis
Diagnosis of MDS dependent on:
Quantitative changes in blood elements (
cytopenias
)
Evidence of dysplasia in peripheral blood smear and marrow
HistorySigns and symptoms Past medical history + comorbiditiesBlood transfusion historyPrior chemotherapy/radiation treatmentFamily historyMedicationsExposure to chemicals
Physical ExamInvestigating for evidence of cytopenias
Integumentary
Mucous membranes
Bleeding- epistaxis, gum bleeding, hemoptysis, hematuria, prolonged menstruation, melena
Fatigue
Vital signs
Presence of fevers, infections
Presence of splenomegaly
Slide11Diagnostic Investigations
Slide12WHO Classification of MDS
Subtype
Peripheral
blood
Bone marrow
% blasts
Refractory anemia
Anemia
Unilineage
erythroid
dysplasia
(in >10% cells)
<5
Refractory
neutropenia
Neutropenia
Unilineage
granulocytic
dysplasia
<5
Refractory thrombocytopenia
Thrombocytopenia
Unilineage
megakaryocytic dysplasia
<5
Refractory anemia with ring
sideroblasts
(RARS)
Anemia
Unilineage
erythroid
dysplasia
>15%
erythroid
precursors are ring
sideroblasts
<5
Refractory
cytopenia
with
multilineage
dysplasia (RCMD)
Cytopenia
Multilineage
dysplasia +/- ring
sideroblasts
<5
Refractory
anemia with excess blasts type 1 (RAEB-1)
Cytopenia
Unilineage
or
multilineage
dysplasia
5-9
Refractory anemia with excess blasts type
2 (RAEB-2)
Cytopenia
Unilineage
or
multilineage
dysplasia
10-19
MDS associated
with isolated del (5q-)
Anemia, normal
or high platelet count
5q31 deletion, anemia,
hypolobulated
megakaryocytes
<5
Slide13IPSS-R
Parameter
Categories and Associated Scores
Cytogenetic risk group
Very good
Good
Intermediate
Poor
Very poor
0
1
2
3
4
Marrow
Blast proportion
≤2%
>2-<5%
5-10%
>10%
0
1
2
3
Hemoglobin
≥10g/
dL
8-<10g/
dL
<8 g/
dL
0
1
1.5
ANC≥0.8 x 109/L<0.8 x 109/L00.5Platelet Count≥100 x 109/L50 - 100 x 109/L<50 x 109/L00.51
Tool is only helpful at time of diagnosisTool is used to estimate life expectancy for NEWLY diagnosed patients with MDS
Risk Category
Risk
Score
Very low
≤1.5
Low
>1.5-3
Intermediate
>3-4.5
High
>4.5-6
Very high
>6
Slide14IPSS-R
Slide15Prognosis
Factors that predict outcome include:
WHO classification
Complex karyotype (>3 chromosome abnormalities)
Chromosome abnormalities
Blast proportion
Cytopenias Even low risk MDS has significant morbidity and mortality including transfusion requirements and associated complicationsWorsening of pancytopenia, acquisition of chromosomal abnormalities, increase in number of blasts are poor prognostic indicatorsTherapy related MDS is an extremely poor outlook
Slide16Treatment
Dependent on:
Patient’s age
Performance status
Prognostic score
WHO classification comorbidities
Determine treatment goals with patient and family, including achieving hematologic improvement, reducing transfusion requirements, delaying transformation to leukemia, improving survival and maintaining quality of lifeDevine, 2013
Slide17Low Risk MDS Treatment Options
(IPSS Low Risk/
Int
Risk-1)
For patients that are
asymptomatic
watchful waiting and monitor Q3-6 monthsSymptomatic Treatment optionsMedications for anemia (ESA, lenalidomide), neutropenia (antibiotics, GCSF), thrombocytopenia (
antifibrinolytics)Immunosuppressive therapy (ATG, Cyclosporine)
Supportive Care (transfusion support, iron chelation)
Allo
-SCT assessment
Delayed
allo
-SCT offers maximal life expectancy as long as transplant occurs before transformation to leukemia
Eligibility ultimately decided by transplant center
Often SCT is not an option to due to patients’ older age or comorbidities
Mdsclearpath.org
Slide18Disease Progression
Potential indicators of progression to high risk MDS
Worsening
cytopenia
New
cytopeniaAppearance of blasts
Rising LDHSystemic symptoms (fever, weight loss)Specific evaluation of higher risk MDSBone marrow aspiration and biopsyFlow cytometryCytogenetics
Mdsclearpath.org
Slide19Treatment Options for High Risk MDS
Goal of treatment:
Change natural history of MDS
Defer AML transformation
Improve survival for patients with MDS
Treatment Options:
Hypomethylating agents (azacitidine, decitabine) (usually standard of care, however not a cure for MDS)Chemotherapy Allogeneic Stem Cell TransplantSupportive Care/ Palliative CareClinical TrialMdsclearpath.org
Slide20Supportive Care
All patients should receive supportive care as it is adjunct to chosen therapy
Patients with
cytopenias
and associated symptoms can receive supportive care
Transfusion support
Red cells or plateletsCMV negativeNursing Management: Identify symptoms of anemia, monitor CBC, monitor for fluid overload and advocate for diureticAssess response to platelet transfusions (platelet refractoriness) and PRBCS (Hgb)Monitor for SE of transfusionsIron overload
Mdsclearpath.org
Slide21Iron Overload Management
Iron Chelation Therapy
Deferoxamine
SC daily dose of 1,000–2,000 mg (20–40 mg/kg/day) should be administered over 8–24 hours, using a small portable pump capable of providing continuous mini-infusion.
SE: allergic reaction, ocular and ototoxicity, cardiac dysfunction
pretreatment hearing and visual exam
Defersirox Initial dose 20 mg/kg body weight daily, orally, taken on an empty stomach 30 minutes prior to meals. SE: GI hemorrhage, hepatic/renal failure, cytopenias
, diarrhea, n/v, abdo pain
Deferiprone
SE: agranulocytosis
Measure ANC, interrupt if ANC <1.5
Slide22Impact of MDS on Patients/Families
Quality of life is complex, individually defined for patients living with MDS
Includes physical, social, emotional, practical and spiritual aspects
Aging, comorbidities, fatigue, and uncertain illness trajectory affects the quality of life of patients
Oncology nurses are in an appropriate position to monitor the impact of the illness and treatment on patients and their quality of life through systematic assessment, providing appropriate interventions, referrals and ongoing support
Thomas,
Crisp & Campbell,2012
Slide23Aplastic Anemia
Pancytopenia (low blood counts) as a result of hypoplasia of bone marrow
Can be inherited or acquired, majority are acquired
Reduction in number of hematopoietic stem cells and an immune reaction or error in the remaining stem cells causing them to not divide or differentiate appropriately to populate bone marrow
Image: Medical-dictionary.thefreedictionary.com;
Hoffbrand
& Moss, 2016
Slide24Prevalence and Etiology
Affects primarily children (with children, majority are inherited), young adults or adults >60
More common in people of Asian descent
2-12 new cases/million each year
Etiology:
Inherited or acquired
Most cases are idiopathicExposure to chemicals, drugs, viruses, radiation, immune diseasesIncekol & Ghadimi, 2015; Hoffbrand & Moss, 2016
Slide25Clinical Features
Present with signs and symptoms of pancytopenia
Most frequent symptoms:
Bruising
Bleeding gums
Epistaxis
Menorrhagia Symptoms of anemia (Pallor, headache, palpitation, SOB/dyspnea, fatigue, foot swelling)Infections are common and frequently life threatening Incekol
& Ghadimi, 2015; Hoffbrand & Moss, 2016
Slide26Diagnosis
Blood work
CBC with diff, B12, folic acid, LFT, LDH,
chem
panel,
coagsPancytopenia early on
Bone Marrow Aspirate and BiopsyBone marrow is profoundly hypocellular, marrow space is composed mostly of fat cells and marrow stroma Flow cytometry To detect coexisting disordersCytogenetics
Rule out MDS and congenital disorders
Slide27Classification
Slide28Treatment
very
severe & severe aplastic anemia stages require treatment as this category has a high mortality
rate
HCT
(
hematopoeitic stem cell therapy)Dependant on age, functional status and availability of donorImmunosuppressive therapyATG (Antithymocyte globulin)Horse ATG administered IV over 4 daysRequires pre-medication with tylenol
/ benadryl to decrease infusion reactions and serum sickness reactionRequires daily steroids to reduce risk of serum sickness
Risk for anaphylaxis- keep anaphylaxis kit at bedside during infusion
Cyclosporine
SE: HTN, renal insufficiency, Mg deficiency, gum hyperplasia
Requires BP, Cr monitoring, regular dental care
Larratt
,
powerpoint
; Longo, 2017
Slide29Serum Sickness
Occurs 1-2 weeks after initiating treatment of ATG
F
lu-like illness, rash and arthralgia
Treatment: steroids
Slide30Supportive Care
Transfusions
RBC, platelets
Irradiated Blood
Treatment of Infections
Empiric therapy with broad spectrum antibioticsGrowth factors as prophylaxis for repeated infections
Infection Prevention and MonitoringPatient education on preventing infections and monitoring for fever and signs and symptoms of infection
Slide31Paroxysmal Nocturnal
Hemoglobinuria
(PNH)
Acquired hemolytic anemia
Characterized by:
Longo, 2017
Slide32Pathophysiology
Acquired mutation in PIG-A gene in hematopoietic stem cell
If mutation proliferates the result is a clone that is deficient in cell surface proteins known as
glycosylphospatidylinositol
-anchored proteins (GPI-AP)
The GPI-AP proteins act as receptors, complement regulators and adhesion molecules
CD55 and CD59 which are two GPI-AP that protect red blood cells from complement activity are not present on the surface of the PNH red blood cells, which leaves these cells extremely sensitive to complement-mediated destruction Young et al., 2009
Slide33Prevalence
Same frequency in men and women
Rare disease
Prevalence estimated at 5/1,000,000
Can present in small children or older adults, most patients are young adults
Slide34Clinical Presentation
Brodsky, 2014
Slide35Diagnosis
Blood work
CBC with diff
Liver profile, bilirubin
LDH
Reticulocyte countUrinalysis
HemoglobinuriaFlow CytometryIdentify the GPI-AP deficient peripheral blood cells Parker et al., 2005
Slide36Treatment
Supportive Care
Transfusions
Folic acid/iron supplements
Treatment of complications (
eg. Thrombosis)
BiotherapyEcullizumab (Solaris) Allogenic SCT for young patient with severe PNHPrimary prophylaxis for thrombosisLongo, 2017
Slide37Nursing Considerations for Bone Marrow Failure Diseases
Comprehensive assessment of patient and management of side effects
Monitoring for signs and symptoms of
cytopenias
including fatigue, bleeding, infection, etc
.
and providing appropriate interventionsAddressing patient’s supportive care needsEducation for patients and families on understanding the disease and its manifestations, treatment modalities and the adverse effects from treatment Connect to hospital and community resources
Slide38AAMAC
Telephone and e-mail patient-to-patient support
Educational material on Aplastic Anemia, MDS & PNH
Quarterly newsletter
Patient Tracker
Local support group meetings
Grants for medical research and educationWebsite, Facebook, Marrowforums
http://www.aamac.ca/
Slide39References
Devine, H. (2013).
Myelodysplastic
syndromes. In M. Olsen & L.
Zitella
(Eds.), Hematologic Malignancies in Adults
(51-74). Pittsburgh, Pennsylvania: Oncology Nursing Society.Buckstein, R. & Wells, R. (2008). Myelodysplastic syndromes (MDS). Retrieved from: https://sunnybrook.ca/uploads/Myelodysplastic_Syndromes.pdfBurgoyne, T. & Knight, A. (2000). Myelodysplastic syndromes. In M. Grundy (Ed.), Nursing in Hematological Oncology (21-30). London, UK: Baillere Tindall Royal College of Nursing
Celgene. (2010). Vidaza azacitidine for injection.
Thomas, M.L., Crisp, M., & Campbell, K. (2012). The importance of quality of life for patients living with
myelodysplastic
syndrome.
Clinical Journal of Oncology Nursing,
16(3), 47-57
Van de
Loosdrecht
, A. A., &
Westers
, T. M. (2014). Flow
Cytometric
Immunophenotyping
in
Myelodysplasia
: Discovery and Diagnosis. Blood, 124(21), SCI-24. Accessed June 24, 2018. Retrieved from http://www.bloodjournal.org/content/124/21/SCI-24.
Incekol
, D. &
Ghadimi
, L. (2015). Princess Margaret cancer
centre
: malignant hematology: self-learning booklet. 3
rd
edition.
Longo, D.L. (2017). Harrison’s hematology and oncology. New York: McGraw-Hill Education
Brodsky, R. A. (2014). Paroxysmal nocturnal
hemoglobinuria. Blood, 124, 2804-2811Parker, C. et al. (2005). Diagnosis and management of paroxysmal nocturnal hemoglobinuria. Blood, 106, 3699-3709Young, N.S. et al. (2009). The management of paroxysmal nocturnal hemoglobinuria: recent advance in diagnosis and treatment and new hope for patients. Seminars in Hematology, 46(1), S1-S6
Slide40References
Hoffbrand
, A.V. & Moss, P. A.H. (2016).
Hoffbrand’s
Essential
Haematology. West Sussex, UK: Wiley & Sons, Ltd.MDS Clear Path. Mdsclearpath.org
Scheinberg, P., DeZern, A.E. & Steensma, D.P. (2016). Acquired bone marrow failure syndromes: aplastic anemia, paroxysmal hemoglobinuria, and myelodysplastic syndromes. Retrieved from: http://ash-sap.hematologylibrary.org//content/2016/489.extract?utm_source=TrendMD&utm_medium=cpc&utm_campaign=American_Society_of_Hematology_Self-Assessment_Program_TrendMD_0
Young NS. Young N.S. Young, Neal S.Bone Marrow Failure Syndromes Including Aplastic Anemia and Myelodysplasia. In: Kasper D, Fauci
A, Hauser S, Longo D, Jameson J,
Loscalzo
J. Kasper D,
Fauci
A, Hauser S, Longo D, Jameson J,
Loscalzo
J Eds. Dennis Kasper, et
al.eds
.
Harrison's Principles of Internal Medicine, 19e
New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com/Content.aspx?bookid=1130§ionid=79731602. Accessed August 01, 2018
.
Zhang, L. (2016). Inherited and acquired bone marrow failure syndromes: in the era of deep gene sequencing.
Journal of Leukemia, 4
(4)