
513 Chapter 22 GOALS AND MECHANICS OF CARDIOPULMONARY BYPASSThe cardiopulmonary bypass CPB circuit is designed to perform four major functions 1 oxygenation and carbon dioxide elimination 2 ci ID: 938583
Download Pdf The PPT/PDF document "Cardiopulmonary Bypass and the Anesthes..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






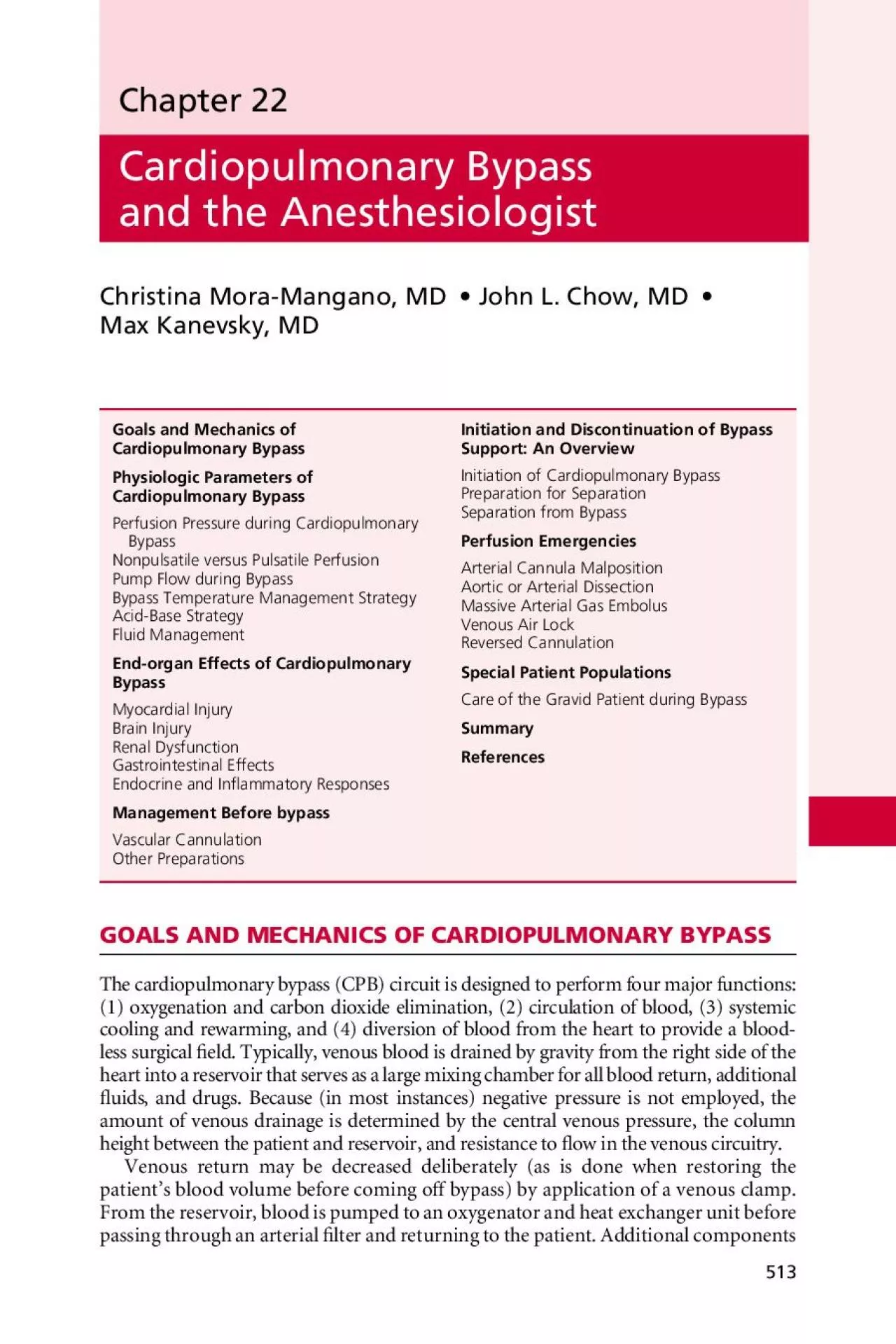
513 Chapter 22 Cardiopulmonary Bypass and the AnesthesiologistChristina Mora-Mangano, MD• John L. Chow, MD• Max Kanevsky, MD GOALS AND MECHANICS OF CARDIOPULMONARY BYPASSThe cardiopulmonary bypass (CPB) circuit is designed to perform four major functions: (1) oxygenation and carbon dioxide elimination, (2) circulation of blood, (3) systemic cooling and rewarming, and (4) diversion of blood from the heart to provide a blood-less surgical eld. Typically, venous blood is drained by gravity from the right side of the heart into a reservoir that serves as a large mixing chamber for all blood return,additional uids, and drugs. Because (in most instances) negative pressure is not employed, the amount of venous drainage is determined by the central venous pressure, the column height between the patient and reservoir, and resistance to ow in the venous circuitry.Venous return may be decreased deliberately (as is done when restoring the patient’s blood volume before coming off bypass) by application of a venous clamp. From the reservoir, blood is pumped to an oxygenator and heat exchanger unitpassing through an arterial lter and returning to the patient. Additional components Cardiopulmonary BypassCardiopulmonary BypassEnd-organ Effects of Cardiopulmonary Management Before bypassReferences VEXTRACORPOREAL CIRCULATION514 of the circuit generally include pumps and tubing for cardiotomy suction, venting, and cardioplegia delivery and recirculation, as well as in-line blood gas monitors, bubble detectors, pressure monitors, and blood sampling ports. A schematic repre-The cannulation sites and type of CPB circuit used are dependent on the type of operation planned. Most cardiac procedures use full CPB, in which the blood is drained from the right side of the heart and returned to the systemic circulation through the aorta. The CPB circuit performs the function of heart and lungs. Aor-toatriocaval cannulation is the preferred method of cannulation for CPB, although femoral arteriovenous cannulation may be the technique of choice for emergency access, repeat sternotomy, and other clinical settings in which aortic or atrial can-nulation is not feasible. Procedures involving the thoracic aorta are often performed using partial bypass in which a portion of oxygenated blood is removed from the left side of the heart and returned to the femoral artery. Perfusion of the head and upper extremity vessels is performed by the beating heart, and distal perfusion is provided below the level of the cross-clamp by retrograde ow by the femoral artery. All blood The primary objective of CPB is maintenance of systemic perfusion and respiration. Controversy arises with the question of whether systemic oxygenation a
nd perfu-sion should be “optimal or maximal.” Remarkably, after more than one-half century Figure 22-1 Components of the extracorporeal circuit: (1) integral cardiotomy reservoir; (2) membrane oxygenator bundle; (3) venous blood line; (4) arterial blood line; (5) arterial lter purge line; (6) arterial line lter; (7) venous blood pump (also called the arterial pump head; this pump forces venous blood through the membrane oxygenator and arterialized blood to theaortic root); (8) cardiotomy suction pump; (9) ventricular vent pump; (10) cardioplegia pump; (11) crystalloid cardioplegia; (12) water inlet line; (13) water outlet line; and (14) gas inlet line. (From Davis RB, Kauffman JN, Cobbs TL, Mick SL: Cardiopulmonary Bypass. New York, Springer-Verlag, 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST515 of CPB, there is continued disagreement regarding the fundamental management of extracorporeal circulation. Clinicians and investigators disagree on what are the best strategies for arterial blood pressure goals, pump ow, hematocrit, temperature, blood gas management, or mode of perfusion (pulsatile vs. nonpulsatile) (Box 22-1Additional considerations of what is best relate to other goals of CPB: maintenance of Perfusion Pressure during Cardiopulmonary BypassSelection of perfusion pressure during CPB is based on balancing the demands of surgical access (bloodless eld) with patient outcome (adequate oxygen delivery). Lower ow and pressure during CPB may optimize visualization, whereas higher ow and pressure may minimize patient complications. Determining the optimum perfusion pressure has been extremely challenging because no single study can adequately address all the complexities of CPB. Because of the brain’s poor toler-ance of ischemia, neurologic outcome has been the most common outcome studied in relation to perfusion pressure. The complicated relationship between neurologic outcome and perfusion pressure is likely related to two causes of adverse neurologic Between mean arterial pressures (MAP) of 50 and 150 mmHg, cerebral auto-regulation maintains a relatively constant blood ow and oxygen delivery. During hypothermic CPB, the lower limit of cerebral autoregulation may be as low as 20 to 30 mmHg, affording some additional protection against hypoperfusion. Increasing perfusion pressure to alleviate the risk of hypoperfusion may lead to greater embolic load and worse outcomes. Ultimately, the selection of perfusion pressure during CPB Subgroups at increased risk for adverse outcomes that may bene t from higher perfusion pressure during CPB include patients with severe atheromatous disease (cerebrovascular or aortic arch), advanced age, systemic hypertension, and d
iabetes. Increased cerebral dysfunction in the elderly may be a result of slower vasodilatation of cerebral resistance vessels during periods of rewarming and subsequent transient episodes of metabolism- ow mismatch with resultant ischemia. It is unknown what the effect of elevating perfusion pressure during rewarming would be on neurologic outcome. Hypertensive patients are generally accepted to have intact pressure- ow autoregulation, with a rightward shift in the cerebral autoregulation curve such that pressure-dependent ow patterns develop at higher perfusion pressures than in the normal population. In hypertensive patients the use of higher perfusion pressure during CPB is common practice. Patients with type 1 diabetes mellitus appear to have impaired metabolism- ow coupling during CPB. They also have some loss of Practice VEXTRACORPOREAL CIRCULATION516 Once the CPB team has selected target perfusion pressures during CPB, a few technical issues emerge. Throughout this discussion perfusion pressure and MAP have been used almost interchangeably. In general, cerebral perfusion pressure is what is of most concern. Cerebral perfusion pressure is determined by the differ-ence between MAP and the higher of central venous pressure and intracranial pres-sure. The latter values are usually less than 5 mmHg during CPB. However, in the presence of compromised cerebral venous drainage (malpositioned cannula, patient Measurement artifacts also play a role in perfusion pressure management. MAP may vary by as much as 20 mmHg over 30 seconds while pump ow is constant. The mechanism of this oscillation and its relation to outcome are unclear. A more common artifact is discordance between radial arterial and central arterial pressures during rewarming. This difference may be as great as 30% and is believed to occur After acknowledging the technical issues of pressure monitoring, the CPB team is left to maintain the selected perfusion pressure. To achieve these perfusion pres-sure goals the team has two general options: alterations of pump ow or adminis-tration of vasoactive agents. Increasing pump ow may be used as a temporizing measure for hypotension if surgical demands allow it; however, this may come at the cost of dangerously reducing reservoir volume. Alternatively, phenylephrine and norepinephrine may be used to support perfusion pressure. In the case of hyperten-sion, pump ow may be reduced, although this increases the potential for inadequate oxygen delivery; more commonly, a vasodilator, such as sodium nitroprusside or nitroglycerin, is employed. Iso urane or another volatile anesthetic may be admin-istered through the pump oxygenator, with careful attention paid to its u
se during It remains uncertain whether pulsatile CPB improves outcome compared with stan-dard, nonpulsatile CPB. Claims of advantages to pulsatile ow are effectively offset The comparatively small size of the arterial in ow cannula can effectively lter out a large component of the pulsatile kinetic energy. Consequently, as achieved clini-cally, pulsatile ow may actually be quite similar energetically to nonpulsatile ow. This potentially unrecognized lack of difference in types of ow may partly explain Like perfusion pressure, pump ow during CPB represents a careful balancethe con icting demands of surgical visualization and adequate oxygendelivery. Two theoretical approaches exist. The rst is to maintain oxygen delivery during bypass at normal levels for a given core temperature. Although this may limit hypoperfusion, it does increase the delivered embolic load. The second approach is to use the low-est ows that do not result in end-organ injury. This approach offers the potential advantage of less embolic delivery as well as potential improved myocardial protec-During CPB, pump ow and pressure are related through overall arterial imped-ance, a product of hemodilution, temperature, and arterial cross-sectional area. This is important because the rst two factors, hemodilution and temperature, are critical 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST517 determinants of pump ow requirements. Pump ows of 1.2 L/min/m perfuse most of the microcirculation when the hematocrit is near 22% and hypothermic CPB is being employed. However, at lower hematocrits or periods of higher oxygen con-Most perfusion teams also monitor mixed venous saturation, targeting levels of 70% or greater. Unfortunately, this level does not guarantee adequate perfusion of all tissue beds, because some (muscle, subcutaneous fat) may be functionally removed from circulation during CPB. Hypothermic venous saturation may overestimate end-organ reserves. Regional perfusion of various end-organs (brain, kidney, small intestine, pancreas, and muscle) has been quanti ed with a uorescent microsphere Cerebral blood ow was unchanged at higher pump ows. Renal perfu-sion was maintained at ows of 1.9 and 1.6 L/min/m. Perfusion to the pancreas was constant at all ows, and small bowel perfusion varied linearly with pump ow. During CPB, most of the outcomes studied in relation to pump ow are those related to the organs at high risk for ischemic injury (i.e., kidney and brain). Much work has been applied to examining the relationship between renal dysfunction and pump ow. Preexisting renal disease is a consistent predictor of postoperative renal dysfuncti
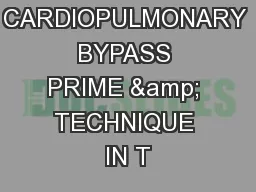
on, the incidence of which ranges between 3% and 5%. Renal func-tion appears unaltered when pump ows greater than 1.6 L/min/m are employed, but whether this management will affect outcomes in patients with preexisting renal Bypass Temperature Management Although hypothermic temperatures have been employed since the advent of extra-corporeal circulation, the importance of reduced temperatures during bypass was The brain is arguably the organ most vulnerable to ischemic damage during CPB. Cerebral hypoperfusion and embolic phenomena are likely to occur in every patient undergoing bypass, resulting in ischemic events. It is believed that hypothermia provides protection from ischemic phenomena and resultant infarction by decreas-ing cerebral oxygen demands, maintaining energy (ATP, phosphocreatine) stores. Although the effect of reduced temperatures on metabolism is of importance, there is increasing evidence that the most important salutary effects of hypothermia on cerebral ischemia are not related to the reduction in metabolism but rather to the Several groups of investigators have assessed the effect of normothermic tempera-tures during bypass on perioperative central nervous system events in cardiac surgery Mild hypothermia provides some magnitude of cerebral protection during CPB, whereas mildly hyperthermic temperatures �(37°C) exacerbate and amplify the Because the brain is vulnerable to hyperthermic temperatures, it is important to use the temperature-monitoring site most likely to re ect cerebral temperature. The most commonly used sites in cardiac surgery patients include esophageal, nasopharyngeal, tympanic, pulmonary arterial, rectal, urinary bladder, subcutaneous (or muscle), and cutaneous sites. Unfortunately, none of these monitoring VEXTRACORPOREAL CIRCULATION518 has been demonstrated to re ect cerebral temperature reliably. With exposure of the brain, investigators have placed a thermocouple directly in the cerebral cortex. Brain temperature was compared with values obtained from sensors in eight locations.Investigators found a poor concordance between cerebral temperature and values obtained at the other monitoring sites. Locations hypothesized to best re ect core temperature—tympanic membrane, esophagus, nasopharynx, pulmonarysometimes overestimated cerebral temperature or underestimated brain tempera-ture. Because of the substantial variability noted in central temperature readings Fig. 22-2) and lack of the concordance of central temperature measures in every patient, the investigators recommended the use of at least three measures of central The management of acid-base status during hypothermic CPB has been a long-standing source of debate. Understanding of the physiologi
c responses to hypo-thermia, and the in uences of Pco have led to shifts in clinical practice over the past decades. Two strategies exist for managing acid-base balance during Temperature (°C)Peripheral sitesPatient #18Circulatory Figure 22-2 Graphic depiction of temperature-time relationship during cardiopulmonary bypass and deep hypothermic circulatory arrest. Temperatures are plotted every minute. Central sites are the nasopharynx, tympanic membrane, esophagus, and pulmonary artery. Peripheral sites are the bladder, rectum, axilla, and sole of the foot. The two slowest cooling central sites were tympanic membrane and esophagus. (From Stone JG, Young WL, Smith CR, et al: Do standard monitoring sites re ect true brain temperature when profound hypothermia is rapidly induced and reversed? 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST519 periods ofhypothermia: -stat and pH-stat. The term -stat was rst proposed todescribe the theory that acid-base regulation in vertebrate animals functioned during temperature uctuation to maintain a constant ratio () of dissociated to undissociated forms of the imidazole ring on histidine. It is this protein charge state that is important in regulating pH-dependent cellular processes. Hypother-mia increases the solubility of oxygen and carbon dioxide in the blood, leading to a decrease in Pco and an increase in pH at lower temperatures. With -stat blood gas management, the uncorrected (37°) pH is kept at 7.40 with the Pco at 40 mmHg, creating a relative alkalosis at the patient’s actual body temperature. This strategy is considered to be physiologic because the ionization state of histi-dine is unchanged over all temperature ranges and protein structure and function are preserved.The pH-stat approach to acid-base balance maintains a pH of 7.40 and Pcoof 40 mmHg when corrected for body temperature, typically requiring the addition of CO during hypothermic CPB. This method of blood gas manage-ment was generally favored until the mid 1980s because it was believed that the potent vasodilatory effects of CO would provide increased cerebral blood flow and thereby minimize the risk of cerebral ischemia during CPB. It is now recog-nized that pH-stat management during hypothermia produces passive cerebral vasodilation, impairs autoregulatory responses to blood pressure changes and metabolic demands in the brain, and does not improve overall oxygen balance. In contrast, -stat management preserves autoregulation and the relationship between cerebral blood flow and metabolism. Neither blood gas strategy has any significant effect on hypothermic cerebral metabolism. The increased CBF seen with pH-stat may also increase the risk of cerebral embolization or produce a steal p
henomenon.The choice of uid for priming the extracorporeal circuit in CPB remains controversial. The idea of using nonblood prime was rst introduced in 1959. This technique of hemodilution was found to be safe when combined with hypother-mia to reduce oxygen consumption and demand. The use of nonblood primes and moderate hemodilution for CPB has become routine in most centers. A reduc-tion in hematocrit from 40% to 20% allows cooling to 22°C without an increase in blood viscosity or required driving pressure. Hematocrit reduction may be achieved before bypass by means of acute normovolemic hemodilution in the hope ofreinfusing the patient’s own heparin-free blood, rather than allogeneic red blood cells, after CPB.Several studies have investigated the differences between colloid and crystalloid priming solutions. In general, crystalloid solutions lead to decreased colloid osmotic pressure with a resultant increase in extracellular water retention, irrespective of the osmolarity of the pump prime. Albumin, unlike a pure crystalloid prime, can decrease the interaction of blood components with the bypass circuit by coating the uid pathway surfaces. In their meta-analysis of 21 controlled trials enrolling 1346 patients, Russell and associates showed a notably smaller drop in on-bypass Ultra ltration during bypass can be used as a means of reducing excessaccumulation. Modi ed ultra ltration describes the process of hemo ltration immediately after the cessation of bypass. This process results in a more consistent reduction in total body water with signi cant increases in hematocrit, myocardial VEXTRACORPOREAL CIRCULATION520 Myocardial InjuryMost coronary revascularization procedures are completed with the assistance of CPB. Although the completion of coronary anastomoses is facilitated by CPB(i.e., the surgeon can operate on a quiet, nonbeating heart), the heart is subjected to a series of events leading to ischemic myocardium during extracorporeal circulation. The operation, which is designed to preserve and improve myocar-dial function, is sometimes associated with myocardial damage (Box 22-2). The extent and incidence of this injury are dependent on the sensitivity and specific-ity of the diagnostic methods being used. However, most patients who undergo cardiac operations sustain some degree of myocardial injury. Although patients with normal ventricular function may tolerate these minor amounts of injury without detectable sequelae, those with impaired ventricular function preopera-tively may not be able to tolerate the slightest injury. As the patient population for CPB continues to become older and have greater degrees of concomitant illness, understanding the physiology of an
d developing effective preventive strategies for myocardial injury during CPB are increasingly important. Because myocar-dial damage influences early and long-term results, the identification and con-trol of factors associated with myocardial injury are critical to ensuring good outcomes. Although injury may be linked to anesthetic and surgical manage-ment, myocardial injury usually is thought to occur from inadequate myocardial protection during CPB.The underlying mechanism for most types of myocardial injuries during CPB is chemia. Ischemia develops when oxygen demand outstrips its supply in the heart. This process involves a complex cascade of events that compromise high-energy phosphate and calcium homeostasis. Many reports con rm the role of high-energy phosphate depletion and intracellular calcium accumulation in the pathogenesis of myocardial damage during ischemia and subsequent reperfusion. Oxidative phosphorylation ceases when the tissue Po falls below 5 to 10 mmHg. Then cre-atinephosphate (CP) and anaerobic production become the main sources of high-energy phosphate. These mechanisms are unfortunately limited. Creatine kinase (CK)–mediated transfer of high-energy phosphate from CP to adenosine diphos-phate (ADP) provides animmediate source of energy; the amount of adenosine triphosphate (ATP) produced by transfer is limited initially by substrate availabil-ity and subsequently by lactate inhibition. Anaerobic production is inef cient and self-limiting because of accumulation of metabolites (i.e., lactate, pyruvate, and hydrogen ions) with inhibition of enzyme systems. As high-energy phosphate stores End 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST521 become depleted, the cardiac cells are no longer able to maintain normal transport of calcium out of the cell. Energy-dependent mechanisms that lower intracellular ionized calcium concentration and terminate the contractile process fail because of a lack of high-energy phosphate. The cytosolic concentration of ionized calcium remains high, and energy use persists with the formation of rigor bonds between the contractile proteins. Continued energy use with calcium and proton-activated release of destructive lipoprotein lipase eventually leads to loss of cell integrity and function.Certain speci c events during CPB are associated with myocardial ischemia and injury (Table 22-1). These events lead to ischemia by increasing oxygendemands, decreasing oxygen supply, or a combination of both. When thesefactors are pres-ent together they potentiate myocardial damage. For example, the distended, brillating ventricle with a low perfusion pressure is particularly susceptible to damage.Aortic cross-clamping, potentially a major cause of
myocardial injury during CPB, was a product of evolution. Initially, continuous aortic or direct coronary artery perfusion of the empty, beating heart was used to “protect” the myocar-dium during cardiac repairs. Ventricular fibrillation was frequentlyinduced and maintained to “quiet” the heart and thereby improve exposure and prevent air embolism. Despite continuous perfusion, myocardial damage commonly occurred. Although myocardial protection improved with the addition of mod-erate cardiac hypothermia (28° to 32°C), operating conditions did not. Most surgeons found it difficult toperform precise repairs on the firm, bleeding, beat-ing, or fibrillating heart. Toimprove exposure and minimize the complications associated with direct coronary cannulation for aortic valve replacement (AVR), myocardial ischemia was induced by aortic cross-clamping. However, the tech-nique of normothermic or moderate hypothermic ischemic arrest is not without problems. First, the heart continues to beat for some time after application of the aortic cross-clamp, thereby compromising the antcipated improvement in operating conditions. Persistent electrical and mechanicalactivity during much of the ischemic period needlessly depletes high-energy phosphate and compro-mises post-repair ventricular performance. Second, few surgeons can complete a complex repair quickly enough to prevent significant myocardial damage in the unprotected heart. Third, the use of intermittent cross-clamping with periods of reperfusion does little to improve operating conditions or prevent necrosis. Reactive hyperemia after release of the aortic clampcontinues to obscure the Abnormal perfusate compositionPersistent ventricular brillation Factors Associated with Myocardial Injury during Cardiopulmonary Bypass VEXTRACORPOREAL CIRCULATION522 operative field. Multiple short periods of reperfusion, particularly in the pres-ence of VF, may potentiate rather than prevent ischemicdamage. De brillation to improve reperfusion reintroduces the problem of systemic air embolism dur-ing open repairs.Rapid cessation of electrical and mechanical activity immediately after aortic cross-clamping is desirable to potentiate surgical exposure and myocardial preser-vation. The extent of necrosis in unprotected myocardium is directly related to the duration of aortic cross-clamping. The ischemic time should be minimized. Variabil-ity among patients in terms of myocardial vulnerability makes it dif cult topredict safe periods of interval ischemia. Prolonged surgical time demands direct interventions to protect the myocardium. These focus along the lines of maximizing high-energy phosphate production while minimizing high-energy phosphate use and intracellu
lar calcium accumulation during the ischemic period. Speci c interventions adenosine-regulating compounds. Uninterrupted periods of ischemia provide the best operating conditions while minimizing the risk of reperfusion injury and air A favorable metabolic milieu during arrest helps provide a margin of safety modi cation after an ischemic insult can minimize structural and The rst concept includes phenomena under the direct control of the anesthesi-ologist. In the pre-bypass period, the heart should be prepared for ischemic arrest by optimizing myocardial metabolism and providing hemodynamic conditions that Patients coming to cardiac surgery (especially in this era of same-dayadmissions) are frequently dehydrated and hypoglycemic. The anesthesiologist should rehy-drate the patient and administer suf cient glucose to improve the heart’s abil-ity to tolerate ischemic arrest. Because the initiation of bypass is frequently accompanied by hypotension, the anesthesiologist should be prepared to admin-istervasoconstrictive drugs (e.g., phenylephrine) to maintain coronary perfusion pressure. Similarly, ventricular distention must be avoided (especially before bril-latory arrest) because increases in left ventricular end-diastolic pressure decrease coronary perfusion pressures and greatly compromise subendocardial oxygen delivery. The anesthesiologist should monitor intraventricular volume with a trans-esophageal echocardiography (TEE) probe after the initiation of bypass. The sur-geon can prevent ventricular distention by placing a hole in the left atrium, left ventricle, or pulmonary artery or by placing a vent in the left ventricle. Although negative pressure venting enhances the risk of intracavitary air entrapment, many surgeons prefer active venting to passive methods. Several pharmacologic interven-tions administered to patients or added to the cardioplegic solution may enhance myocardial protection. -Receptor antagonists (e.g., propranolol, esmolol) provide myocardial protection by decreasing heart rate and myocardial metabolism. The heart rate should be maintained at less than 80 beats per minute in patients with ischemic heart disease in the pre-bypass period. 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST523 The brain is highly susceptible to injury during CPB. Many clinicians believe that cerebral injuries after cardiac surgery are the most devastating adverse outcomes associated with CPB. A study of 2400 patients undergoing elective coronary artery bypass grafting (CABG) from 24 U.S. centers reported that 6.1% of patients suffer adverse postoperative gross neurologic or psychiatric central nervous system events. These patients remain in the intensive care unit and hospital for gr
eater periods of time, and 1 in every 3 surviving patients does not return home but requires contin-The effects of CPB on the renal system have signi cant health and economic impacts; however, despite intensive investigation into the pathogenesis and prevention of renal failure, there remains limited progress in the development of effective pro-tective strategies in recent decades. Because intravascular volume depletion and hypoperfusion can lead to exacerbation of renal ischemia and accentuate the risk for postoperative acute renal failure, avoidance of nephrotoxic agents and close atten-tion to intravascular volume, blood pressure, and cardiac output (CO) are central in Gastrointestinal EffectsThe effects of CPB on the gastrointestinal system are complex and not fully elucidated. Although most patients undergoing cardiac surgery do not suffer adverse changes in gastrointestinal function, subclinical perturbations including transient elevations in hepatocellular enzymes and hyperamylasemia have been observed after CPB. Although the incidence of gastrointestinal complications after CPB is low (range, 0.3% to 3.7%), they are associated with signi cant morbidity and remarkably high mortality (range, 11% to 67%) compared with cardiac surgery patients without postoperative gastrointestinal compromise. The frequently reported adverse gas-trointestinal outcomes include gastroesophagitis, upper and lower gastrointestinal hemorrhage, hyperbilirubinemia, hepatic and splenic ischemia, colitis, pancreatitis, cholecystitis, diverticulitis, mesenteric ischemia, as well as intestinal obstruction, Although the pathophysiology of gastrointestinal complications after cardiac surgery is likely multifactorial, a unifying mechanism is splanchnic hypoperfusion. The gastrointestinal system is particularly vulnerable for ischemia due to the lack of autoregulation and to the preferential shunting of blood away from the gastroin-testinal circulation during periods of hypotension. Hypothermia and nonpulsatile ow during CPB may be detrimental to mucosal perfusion. However, hypothermia has little effect on hepatic arterial blood ow and may actually increase portal ow. There is no signi cant difference in hepatic blood ow between pulsatile and non-pulsatile perfusion at high ow rates (2.4 L/min/m) during hypothermia. Perhaps more important to the development of inadequate gastrointestinal perfusion is the signi cant increase in total body oxygen consumption in the immediate hours after CPB. Visceral hypotension is the most signi cant factor in the development of gas-trointestinal complications after cardiac surgery. Gut ischemia of suf cient duration impairs gastrointestinal tract barrier function.
Studies evaluating gut permeability have shown that CPB is associated with an increase in mucosal permeability and VEXTRACORPOREAL CIRCULATION524 Cardiopulmonary bypass provokes a marked stress response, which has been quan-ti ed by measurements of hormones and vasoactive substances in plasma. Hypo-thermia, hemodilution, and nonpulsatile ow produce insulin, prostaglandin, and renin release during CPB and are potent stimuli for catecholamine release. Epi-nephrine levels increase throughout CPB with a ninefold increase that peaks during rewarming, after aortic cross-clamp release. Although striking, the magnitude of the catecholamine responses is comparable to that after syncope, myocardial infarction, strenuous exercise, or caffeine ingestion. It is likely that increased plasma catechol-amine concentrations are in part due to decreased clearance. The heart and lungs, which serve as primary clearance organs for these substances, are partially or com-pletely excluded from the circulation during much of CPB. Hypothermia slows all Many other hormones increase during CPB. Vasopressin increases up to 20 times baseline levels during CPB. Some investigators suggest that vasopressin and angio-tensin II are responsible for the elevations in SVR observed during CPB, and this may explain why vasopressin can be a useful drug to increase SVR on CPB in patients who Data from clinical and laboratory investigators now conclusively demonstrate the untoward affects of hyperglycemia in cardiac surgery. Aggressive control of perioper-ative glucose values represents the standard of care in cardiac surgery. Glucose values should be maintained at levels less than 200 mg/dL. Lower values (blood glucose 80 to 120 mg/dL) are likely superior to values of glucose more than 120 mg/dL. A protocol for management of glucose in cardiac surgery patients is outlined in Table 22-212The physiologic insult of CPB results in a myriad of exaggerated, complex, and mostly pathologic immunologic events. The passage of blood through the extracorporeal circuit causes activation of complement, platelets, neutrophils, and proin ammatory kinins. At the conclusion of bypass, blood perturbed by the process of extracorporeal circulation reperfuses ischemic organs, exacerbating the local in ammatory responses in end organs, including the brain, kidney, heart, and lung. These phenomena result in whole-body in ammatory response and represent the collective effect of activa-The complement system is formed by two interconnected cascades: the classi-cal and the alternative pathways. The elements of the classical pathway are C1, C4, and C2, with subunits and fragments of these elements developing as the cascade progresses. The classical pathway is thought
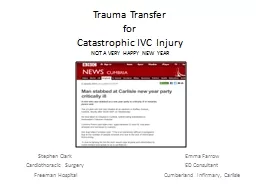
to be normally triggered by antigen-antibody complexes. The alternative pathway, bypassing C1, C4, and C2 to activate C3, is triggered by complex polysaccharides, lipopolysaccharides, IgA and IgD and by exposure of blood to foreign surfaces. The two pathways converge at C3 and lead to activation of the terminal components, C5 to C9. The fragments C3a and C5a are With initiation of CPB, complement is thought to be activated through the alternative pathway. Exposure of blood to the CPB circuit initiates activation of the coagulation cascade by means of the Hageman factor (XII). Although thecoagulation cascade is initiated, it is not completed because of the presence of heparin. Activat-ed factor XII (XIIa) results in plasmin generation. Plasmin activatescomplement by 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST525 C1 (classical pathway), cleaves C3 (alternative pathway), and cleaves factor XII, which activates the kallikrein-kinin systems. Complement activation can also occur through the classical pathway by heparin-protamine complexes. Complement activation leads to direct membrane injury by complement subunits, neutrophil activation, enhance-ment of phagocytosis due to interaction of complement components and phagocytic cells, and release of lysosomal enzymes. The complement fragments are stimulants that induce changes in neutrophil behavior, causing neutrophil activation and migration and the promotion of adhesive and secretory events. These phenomena contribute to the reperfusion injury observed in cardiac surgery patients. Activated neutrophilsattach to the endothelium, causing translocation of P-selectin from intracellular vesicles to the cell membrane and platelet-activating factor (PAF) synthesis. Endothelial membrane-bound PAF leads to increased neutrophil adhesion and activation and neutrophil adhesion protein (CD11/CD18) expression. Ultimately, increases in adhesion molecule emission in the endothelium and other tissue cell types (e.g., myocytes, alveolar cells, glomerular or renal tubular epithelium) result in transmigration of neutrophils into the interstitial space and release of large amounts of free radicals. These phenomena are schematically presented in Figure 22-3 Bolus and start infusion as follows: Blood Glucose (mg/dL) Insulin Bolus Units Measure blood glucose values every 30 minutes intraoperatively! Blood Glucose TreatmentStop insulin; D5W and recheck in 30 min; whenu 150, restart at 50% of previous rate.75-100Stop insulin; recheck in 30 min; restart at 50% of previous rate (unless 0.25 U/hr).101-125If 10% lower than last value, decrease by 0.5 U/hr.If �10% lower than last value, decrease by 50%.If neither, continue current rate.126-175Continue current rate.176-225If lower than las
t value, continue current rate.If higher than last value, increase by 0.5 U/hr.�225 If�10% lower than last value, continue current rate.If10% lower or greater than last value increase by 1 U/hr.If �225 and not decreased after three adjustments, double current rate. Stanford University Adult Cardiac Anesthesia Continuous Insulin Infusion Protocol VEXTRACORPOREAL CIRCULATION526 Although complement has been recognized as a signi cant factor in the develop-ment of the physiologic disturbances seen after cardiac surgery, endotoxins released into the bloodstream during CPB are also believed to play a signi cant role in the in ammatory cascade. Endotoxin binds to lipopolysaccharide-binding protein nor-mally present in serum. This complex binds to speci c receptors on macrophages with subsequent production of cytokines. The collective result of these cellular and humoral responses may be manifest by cardiovascular instability, pulmonary dys-function, renal insuf ciency, alterations in hemostasis, fever, and excess extravascu-Interventions aimed at reducing morbidity associated with the systemic in am-matory response seen after CPB may be directed at preventing or minimizing the activation of the various systems contributing to the response or at blocking the physiologic effects once activation occurs. Studies evaluating membrane versus bub-ble oxygenators have reported con icting data regarding the degree of complement Corticosteroids may play an important role in minimizing theresponse by reducing complement activation, decreasing production ofand interfering with neutrophil adherence and migration. Most clinical trials reported a bene cial effect on markers of in ammation (e.g., cytokine and Ischemia/ReperfusionReleaseof OFRsfrom ECsIncreasedPMN adhesion(P-selectin)PMN activationTight adhesionCD11/CD18 toendothelial cellsICAM-1Transmigration ofPMNs, OFR generation after adherence tointerstitial cellsInductionof cytokinesActivationof PMNsInitialattachmentof PMNsActivationof serumcomplementGeneration ofoxygen free radicalsby PMNs adherentto ECsTissue Injury Figure 22-3 A schematic representation of the interactive components of the immunethat likely occurs during the postischemic in ammatory state after cardiopulmonary bypass. EC = endothelial cells; ICAM = intercellular adhesion molecules; OFR = oxygen free radicals; PMNs = polymorphonuclear leukocytes. (From Herskowitz A, Mangano DT: In ammatory cascade: A nal 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST527 complement levels, histamine release, leukocyte counts, endothelial activation). The use of aprotinin or other protease inhibitors has been shown to produce a dose- dependent reduction in com
plement activation, cytokine release, and neutrophil An important objective of this phase is to prepare the patient for CPB (Box 22-3This phase invariably involves two key steps: anticoagulation and vascular cannu-lation. Heparin is still the anticoagulant clinically used for CPB. Dose, method of administration, and opinions as to what constitutes adequate anticoagulation vary. Heparin must be administered before cannulation for CPB, even if cannulation must be done emergently. Failure to do so is to risk thrombosis in the patient and extra-corporeal circuit. After heparin has been administered, a period of 3 to 5 minutes is customarily allowed for systemic circulation and onset of effect. Various con rma-Vascular CannulationThe next major step in the pre-bypass phase is vascular cannulation. The goal of vas-cular cannulation is to provide access whereby the CPB pump may divert all systemic venous blood to the pump oxygenator at the lowest possible venous pressures and deliver oxygenated blood to the arterial circulation at pressure and ow suf cient to Arterial cannulation is generally established before venous cannulation to allow vol-ume resuscitation of the patient, should it be necessary. The ascending aorta is the preferred site for aortic cannulation because it is easily accessible, does not require an additional incision, accommodates a larger cannula to provide greater ow at arterial cannulation sites (femoral or iliac arteries). Because hypertension increases the risk of aortic dissection during cannulation, the aortic pressure may be tempo-rarily lowered (MAP80 mmHg during aortotomy and cannula insertion). Several potential complications are associated with aortic cannulation, including emboliza-tion of air or atheromatous debris, inadvertent cannulation of aortic arch vessels, Reviews and clinical reports emphasize the importance of embolization as the major mechanism of focal cerebral injury in cardiac surgery patients. Intraopera-tive use of two-dimensional ultrasound to image the ascending aorta as a guide to selection of cross-clamping and cannulation sites is increasing. A femoral artery, rather than the ascending aorta, can be cannulated for systemic perfusion. Management VEXTRACORPOREAL CIRCULATION528 cannulation is used when ascending aortic cannulation is considered relatively con-traindicated, as in severe aortic atherosclerosis, aortic aneurysm or dissection, or known cystic medical necrosis. The anesthesiologist should seek evidence of cannula malposition by looking for unilateral blanching of the face, gently palpating carotid pulses, and checking for new unilateral diminution and by measuring blood pressure Venous cannulation can be achieved using a single atrial can
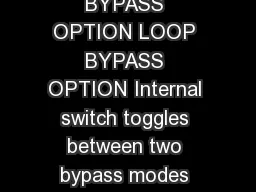
nula that is inserted into the right atrium and directed inferiorly (Fig. 22-4). Drainage holes are located in the inferior vena cava (IVC) and right atrium to drain blood returning from the lower extremities and the superior vena cava (SVC) and coronary sinus, respectively. This technique has the advantage of being simpler, faster and requiring only one incision; however, the quality of drainage can be easily compromised when the heart is lifted for surgical exposure. The bicaval cannulation technique, required in cases in which right atrial (RA) access is needed, involves cannulating the SVC and IVC (Fig. 22-5). Loops placed around the vessels can be tightened to divert all caval blood ow away from the heart. Blood returning to the right atrium from the coronary sinus will not be drained using this technique, so an additional vent or atriotomy is necessary.During CPB, blood will continue to return to the left ventricle from a variety of sources, including the bronchial and thebesian veins, as well as blood that traverses the pulmonary circulation. Abnormal sources of venous blood include a persistent left SVC, systemic-to-pulmonary shunts, and aortic regurgitation. It is important to avoid left ventricular (LV) lling and distention during CPB to prevent myocardial rewarming and to minimize LV wall tension and limit myocardial oxygen demand. This can be accomplished with the use of a vent placed in the pulmonary artery, aortic root, or left ventricle, depending on the likely source of LV blood return.Venous cannulas, using a two-stage or bicaval cannula, are large and can impair venous return from the IVC or SVC. Superior vena caval obstruction is detected by Figure 22-4 Aortic (Ao) and single, double-staged, right atrial (RA) cannulation. Notice the drainage holes of venous cannula in right atrium and inferior vena cava. (From Connolly MW: Car-diopulmonary Bypass. New York, Springer-Verlag, 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST529 venous engorgement of the head and neck, conjunctival edema, and elevated SVC pressure. Inferior vena caval obstruction is far more insidious, presenting only as Femoral venous cannulation is sometimes used to permit partial CPB without, or before, sternotomy or RA cannulation (e.g., repeat sternotomy, ascending aortic aneurysms). Because of their comparatively small size and placement in the distal IVC, femoral venous cannulas do not permit complete drainage of systemic venous blood and only partial CPB may be achieved. A long cannula with multiple fenestra-tions can be inserted through the femoral vein and passed to the level of the IVC-RA Other PreparationsOnce anticoagulation and cannulation are complete, CPB can be instituted. Because there is redundant pulmonary a
rtery (PA) catheter length in the right ventricle, and the heart is manipulated during CPB, there is a tendency for distal migration of the PA catheter into pulmonary artery branches. This distal migration of the catheter increases the risks of “autowedging” and pulmonary artery perforation. During the pre-bypass phase it is advisable to withdraw the PA catheter 3 to 5 cm to decrease the likelihood of these untoward events. It is also advisable to check the integrity of all vascularaccess and monitoring devices. A PAC placed through an external jugular or subclavian vein can become kinked or occluded on full opening of the sternal retractor. If TEE is being used, the probe should be placed in the “freeze” mode and the tip of the scope placed in the neutral and unlocked position. Leaving the electronic scanning emitter on dur-ing hypothermic CPB adds heat to the posterior wall of the ventricle.Before initiating CPB, the anesthesiologist should assess the depth ofanesthesia and muscle relaxation. It is important to maintain paralysis to prevent patientmovement that could result in dislodgment of bypass-circuit cannulae and prevent shivering Figure 22-5 Position of two-vessel cannulation of right atrium (RA) with placement of drainage holes into superior vena cava (SVC) and inferior vena cava (IVC). The aortic cannula is not shown. (From Connolly MW: Cardiopulmonary Bypass. VEXTRACORPOREAL CIRCULATION530 as hypothermia is induced (with the attendant increases in oxygen consumption). It is dif cult to determine the depth of anesthesia during the various stages of CPB. Because blood pressure, heart rate, pupil diameter, and the autonomic nervous system are profoundly affected by extracorporeal circulation (e.g., the heart is asystolic; blood pressure is greatly in uenced by circuit blood ow; sweating occurs withrewarming), these variables do notreliably re ect the anesthetic state. Althoughhypothermia decreases anesthetic requirements, it is necessary to provide analgesia, unconscious-ness, and muscle relaxation during CPB. With the initiation of bypass and hemodilu-tion, blood levels of anesthetics and muscle relaxants will acutelydecrease. However, plasma protein concentrations also decrease, which increases the free-fraction and active drug concentrations. Every drug has a speci c kinetic pro le during CPB, and kinetics and pharmacodynamics during CPB will vary greatly among patients. Many clinicians administer additional muscle relaxants and opioids at the initiation of CPB. A vaporizer for potent inhalation drugs may be included in the bypass circuit. A nal inspection of the head and neck for color, symmetry, adequacy of venous drainage (neck vein and conjunctiva engorge
ment), and pupil equality is reasonable to serve as a baseline for the anesthetic state. A summary of preparatory steps to be accomplished during the pre-bypass phase is given in Table 22-3Initiation of Cardiopulmonary BypassOnce all preparatory steps have been taken, the perfusionist progressively increases delivery of oxygenated blood to the patient’s arterial system, as systemic venous blood is diverted from the patient’s right side of the heart, maintaining the pump’s venous V V Preparation for Bypass: Pre-bypass Checklist 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST531 reservoir volume. After full ow is achieved, all systemic venous blood is (ideally) draining from the patient to the pump reservoir. The central venous pressure (CVP) and pulmonary arterial pressure (PAP) should decrease to near zero (2 to 5 mmHg), whereas systemic ow, arterial pressure, and oxygenation are maintained at desired values. Table 22-4 outlines tasks to be completed within 5 minutes of initiating CPB.Systemic arterial hypotension 30 to 40 mmHg) is relatively common on initiation of CPB. Much of this can be explained by the acute reduction of blood viscosity that results from hemodilution with nonblood priming solutions. MAP increases with initiation of hypothermia-induced vasoconstriction, along with levels of endogenous catecholamines and angiotensin. Treatment with -agonists is not necessary. Of concern is the potential for myocardial and cerebral ischemia Until the aortic cross-clamp is applied, the coronary arteries are perfused with hemodiluted, nonpulsatile blood. If placement of the aortic cross-clamp is delayed, MAP should be maintained in the range of 60 to 80 mmHg to support myocardi-al perfusion, especially in the presence of known coronary stenosis or ventricular hypertrophy. This arterial pressure is likely adequate to maintain cerebral blood ow Preparation for SeparationBefore discontinuation of CPB, conditions that optimize cardiac and pulmonary function must be restored. To a great extent this is achieved by reversing the pro- Checklist for Bypass Procedure VEXTRACORPOREAL CIRCULATION532 It is not uncommon for patients to sweat during rewarming. This is almost certainly caused by perfusion of the hypothalamus (i.e., the thermoregulatory site) with blood that is warmer than the latter organ’s set point (37°C). The brain is a high- ow organ and can be assumed to equilibrate fairly quickly (15 to 20 minutes) with cerebral perfusate temperature (i.e., nasopharyngeal temperature). A less likely but more dis-turbing possibility is that restoration of brain normothermia with decreased anesthetic concentration may result in inadequate depth of anesth
esia and the potential for aware-ness. It is estimated that awareness occurs during cardiac surgery in 1% of patients.Patient movement before discontinuation of CPB is extremely disruptive and may be genuinely life-threatening if it results in cannula dislodgment or disruption of the procedure. Additional muscle relaxant should be administered. If awareness is suspected, supplemental amnestics or anesthetics should be administered dur-ing rewarming. Because sweating stops almost immediately on discontinuation of bypass, continued sweating after emergence from CPB may be a sign of awareness. Neurologic monitors such as the Bispectral Index are being used by some clinicians to help judge the depth of anesthesia during and after weaning from CPB.15When systemic hypothermia is used, body temperature is restored to normother-mia by gradually increasing perfusate temperature with the heat exchanger. Time required for rewarming (i.e., heat transfer) varies with arterial perfusate tempera-ture, patient temperature, and systemic ow. Excessive perfusate heating is not advis-able for at least three key reasons: possible denaturation of plasma proteins, possible V 10. Preparation for Separation-from-Bypass Checklist 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST533 cerebral hyperthermia, and the fact that dissolved gas can condense into bubbles if the temperature gradient is too great. Because small increases (0.5°C) in cerebral tem-perature exacerbate ischemic injury in the brain, it is critical to perfuse the patient with blood temperatures at or below 37°C. Although this will increase the duration of rewarming, the risk of hyperthermic brain injury is greatly increased with hyper-thermic blood temperatures. Many centers employ mild hypothermia (i.e., systemic to 34°C) instead of moderate hypothermia (26° to 28°C), reducing Rewarming may be enhanced by increasing pump ow, which thereby increases heat input. At levels of hypothermia routinely used (25° to 30°C), the patient behaves as if vasoconstricted (calculated SVR is relatively high). Increasing pump ow in this setting may result in unacceptable hypertension. There are two approaches to this problem: wait out the vasoconstriction or pharmacologically induce patient vasodilation. When rectal or bladder temperature approaches 30° to 32°C, patients appear to rapidly vasodilate. This is probably the result of decreasing blood viscos-ity or relaxation of cold-induced vasoconstriction with warming. Increasing pump ow at this point serves several purposes: increased heat transfer, support of sys-temic arterial pressure, and increased oxygen delivery in the presence of increasing oxygen consumption. Of
ten, waiting for the patient to spontaneously “vasodilate” is suf cient; and with subsequent increased pump ows, rewarming will be adequate at separation from bypass support. Circumstances in which more aggressive rewarming may be needed include profound hypothermia with a large hypoperfused “heat sink” Skeletal muscle and subcutaneous fat are relatively hypoperfused during CPB. These tissues cool slowly and are also slow to warm. Temperatures at high- ow regions (e.g., esophagus, nasopharynx) do not re ect the temperature of these tis-sues. Pharmacologic vasodilation allows an earlier increase in pump ow and deliv-ery of warmed arterial blood to low- ow beds, making the rewarming process more uniform. Arteriolar vasodilators (e.g., sodium nitroprusside, hydralazine) are much more likely to be effective in this process than venodilators (e.g., nitroglycerin). Other aids to warming during or after CPB are heating blankets, warmed uids, heated humidi ed gases, and increased room temperature. Sterile forced-air rewarming After aortic cross-clamp release, the heart is again perfused through the native coro-nary arteries. Until the proximal anastomoses are made, myocardial perfusion may be compromised in the presence of a low MAP. Consequently, it is advisable to grad-With discontinuation of CPB, a marked discrepancy often exists between blood pressure readings measured from the radial artery and the central aorta. Radial arte-rial catheters may underestimate central aortic systolic pressures by 10 to 40 mmHg. Discrepancies in MAP tend to be of a lesser magnitude (5 to 15 mmHg). Such a dis-crepancy is not present before CPB, nor is it present after CPB in all patients. Mecha-nisms are unde ned, but evidence supports vasodilatory and arteriovenous shunting At the end of the procedure, intracardiac air is present in virtually all cases that require opening the heart (i.e., valve repair or replacement, aneurysmectomy, septal defect repair, repair of congenital lesions). In such cases, it is important to remove as much air as possible before resumption of ejection. Surgical techniques differ. With VEXTRACORPOREAL CIRCULATION534 the aortic cross-clamp still applied, the surgeon or perfusionist can partially limit venous return and LV vent ow, causing the left atrium and left ventricle to ll with blood. Through a transventricular approach, the left ventricle then can be aspirated. The left atrium and left ventricle are ballotted to dislodge bubbles, and the cycle is repeated. The operating table can be rotated from side to side and the lungs ventilated to promote clearance of air from the pulmonary veins. Rather than transventricular aspiration, some surgeo
ns vent air through the cardioplegia cannula or a needle vent in the ascending aorta. Before removal of the aortic cross-clamp, the patient is placed head down, so that bubbles will oat away from the dependent carotid arteries. Some surgeons favor temporary manual carotid occlusion before cross-clamp removal, but safety and ef cacy of this potentially dangerous maneuver are undocumented. A venting cannula is often left in the aorta at a location that should allow air pickup after resumption of ejection. The aortic cross-clamp can be temporarily reapplied for TEE has shown that routine air clearance techniques are not completely effective. Transcranial Doppler studies document a high incidence of intracranial gas emboli on release of the aortic cross-clamp or resumption of ejection. Three essential ele-ments of air removal are mobilization of air by positive chamber lling, stretching of the atrial wall, and repeated chamber ballottement; removal of mobilized air by Intracardiac air may be present in 10% to 30% of closed cardiac cases as well (e.g., CABG). During aortic cross-clamping, air may enter the aorta and left ventricle retrograde through native coronary arteries opened in the course of CABG surgery, particularly when suction is applied to vent the left side of the heart or aortic root. Efforts to expel air from the left ventricle and aortic root should be routine before unclamping the aorta. It is unclear to what extent gas emboli originating from the heart and aorta contribute to neurologic injury. However, microembolic load cor-relates with magnitude of cognitive dysfunction. Air ejected from the left ventricle can also travel to the coronary arteries, resulting in sudden and sometimes extreme Before discontinuation of CPB, the heart must have an organized rhythm that is spon-taneous or pacer induced. Ventricular brillation (VF), common after cross-clamp release and warming, will often spontaneously convert to some other rhythm. Pro-longed VF is undesirable during rewarming for at least three reasons: (1) subendocar-dial perfusion is compromised in the presence of normothermic VF; (2) myocardial oxygen consumption is greater with VF compared with a beating heart at normother-mia; and (3) if the left ventricle receives a large amount of blood (aortic insuf ciency or bronchial return) in the absence of mechanical contraction, the left ventricle may distend. LV distention increases wall tension and further compromises subendocar-dial perfusion. On the other hand, early resumption of mechanical contraction may make some surgical procedures dif cult (e.g., modi cation of distal anastomoses).De brillation, when necessary, is accomplished with internal paddles at much lower energies th
an would be used for external cardioversion. In the adult, starting energies of 5 to 10 J are routine. De brillation is less effective when the heart has not fully rewarmed, and it is rarely successful if myocardial (perfusate) temperature is less than 30°C. Repeated attempts at de brillation, particularly with escalating energy levels, can lead to myocardial injury. If de brillation is not successful after two to four attempts, options include further warming, correction of blood gas and electrolyte abnormalities if present (high Po and high normal serum potassium [K] seem favor-able), increased MAP, and antiarrhythmic therapy. Bolus administration of 100 mg 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST535 of lidocaine before the release of the cross-clamp signi cantly lowers the incidence of reperfusion ventricular brillation. Increasing coronary perfusion by increased MAP is believed to result in myocardial reperfusion and recovery of the energy state.Before discontinuation of CPB, the lungs must be rein ated. Positive pressure (20 to 40 cmHO) is repeatedly applied until all areas of atelectasis are visually rein ated. Attention is speci cally directed at the left lower lobe, which seems more dif cult to reexpand. Fluid that has collected in the thoracic cavities during CPB is removed by the surgeon; and if the pleural cavity has not been opened, evidence of pneumo-thorax is also sought. The tidal volume or ventilatory rate is increased 10% to 20% above pre-bypass values to compensate for increased Vd/Vt if present. Ventilation is resumed with 100% oxygen and subsequent adjustments in Fio are made based on Correction of Metabolic Abnormalities and Arterial Oxygen SaturationWhen rewarming is nearly complete and separation from CPB is anticipated to occur in 10 to 20 minutes, an arterial blood sample is taken and analyzed for acid-base status, CARRYINGCAPACITYGenerally, a hematocrit of at least 20% to 25% is sought before discontinuation of bypass. The primary compensatory mechanism to ensure adequate systemic oxygen delivery in the presence of normovolemic anemia is increased CO. Increased CO results in an increased myocardial oxygen need, which is met by increased coronary oxygen delivery by coronary vasodilation. The lower limit of the hematocrit, below which increased CO can no longer support systemic oxygen needs, is reported to be 17% to 20% in dogs with completely healthy hearts. With increases in systemic Vosuch as occur with exercise, fever, or shivering, higher values of the hematocrit are required. Patients with good ventricular function and good coronary reserve (or good revascularization) might be expected to tolerate hematocrit values in the 20s. When ventricular
function is impaired or revascularization is incomplete, hematocrit above 25% may aid in support of the systemic circulation and concomitantly lower myo-ARTERIALConsiderable debate has centered on the extent to which acidemia affects myocar-dial performance and whether correction of arterial pH with sodium bicarbonate is advantageous or deleterious to the heart. Most clinical studies have found metabolic acidosis impairs contractility and alters responses to exogenous catecholamines. Hemodynamic deterioration is usually mild above pH 7.2 because of compensatory increases in sympathetic nervous system activity. Attenuation of sympatheticsystem responses by -blockade or ganglionic blockade increases the detrimental effect of acidosis. The ischemic or hypoxic myocardium has been found to be par-ticularly vulnerable to detrimental effects of acidosis. Patients with poor contractile function or reduction of myocardial sympathetic responsiveness (e.g., chronic left ventricular failure), those treated with -blockers, or those with myocardial ischemia are especially susceptible to the adverse effects of acidosis. For these reasons arterial pH is corrected to near-normal levels before discontinuation of CPB, using sodium bicarbonate. Concerns regarding carbon dioxide generation and acidi cation of the intracellular space can be obviated by slow administration and appropriate adjust- VEXTRACORPOREAL CIRCULATION536 ELECTROLYTESElectrolytes most commonly of concern before discontinuation of CPB are potassium and calcium. Serum potassium concentration may be acutely low because of hemo-dilution with nonpotassium-containing priming solutions or large-volume diuresis during CPB. More commonly, potassium concentration is elevated as a result of sys-temic uptake of potassium-containing cardioplegic solution; values exceeding 6 mEq/L are not uncommon. Other potential causes of hyperkalemia that must be considered are hemolysis, tissue ischemia or necrosis, and acidemia. Hypokalemia can be rapidly corrected during CPB with relative safety because the heart and systemic circulation are supported. Increments of 5 to 10 mEq of KCl over 1- to 2-minute intervals can be given directly into the oxygenator by the perfusionist, and potassium subsequently is rechecked. Depending on severity and urgency of correction, elevated potassium can be treated or reduced by any of several standard means: alkali therapy, diuresis, cal-cium administration, or insulin and glucose. Alternatively, hemo ltration can be used to lower serum potassium. While still on CPB, potassium-containing extracellular uid is removed from the patient and replaced with uid not containing potassium.Ionized calcium is involved in the maintenance of normal excitati
on-contraction coupling and therefore in maintaining cardiac contractility and peripheral vascu-lar tone. Low concentrations of ionized calcium lead to impaired cardiac contractil-ity and lowered vascular tone. Concerns have been raised about the contribution of calcium administration to myocardial reperfusion injury and to the action of various inotropes. Some investigators argue in favor of measuring ionized calcium before dis-continuation of CPB and to administer calcium in patients with low concentrations to optimize cardiac performance. Although they routinely measure ionized calcium before discontinuation of bypass, calcium salts are not routinely administered. When confronted with poor myocardial or peripheral vascular responsiveness to inotropes or vasopressors after bypass in the presence of a low level of ionized calcium, calcium salts should beadministered to restore ionized calcium to normal (notelevated) levels in the hope of restoring responsiveness. The same strategy can be used for mea-Before separating from CPB, all monitoring and access catheters should be checked and calibrated. The zero-pressure calibration points of the pressure transducers are routinely checked. Not uncommonly, nger pulse oximeter probes do not have a good signal after CPB. In those cases, a nasal or ear probe is placed to obtain reliable oximetry. Intravenous infusions are restarted before separation from CPB, and their During warming and preparation for separation, an assessment should be made of the functional status of the heart and peripheral vasculature based on visual inspec-tion, hemodynamic indices, and metabolic parameters. Based on this assessment, inotropes, vasodilators, and vasopressors thought likely to be necessary for successful Separation from BypassAfter all preparatory steps are taken, CPB can be discontinued. Venous out ow to the pump or oxygenator is impeded by slowly clamping the venous line, and the patient’s intravascular volume and ventricular loading conditions are restored by transfusion of perfusate through the aortic in ow line. When loading conditions are optimal, the 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST537 At this juncture it must be determined whether oxygenation, ventilation, and more commonly myocardial performance (systemic perfusion) are adequate. A discussion of these issues no longer involves CPB per se but, rather, applied car-diopulmonary physiology. Should separation fail for any reason, CPB can simply be reinstituted by unclamping the venous out ow and arterial in ow lines and restoring pump ow. This allows for support of systemic oxygenation and perfu-sion while steps are taken to diagnose and treat those problems that precluded successful sepa
ration.Accidents or mishaps occurring during CPB can quickly evolve into life-threatening emergencies (Box 22-4). Many of the necessary conditions of bypass (cardiac arrest, hypothermia, volume depletion) preclude the ability to resume normal cardiorespi-ratory function if an accident threatens the integrity of the extracorporeal circuit. Fortunately, major perfusion accidents occur infrequently and are rarely associated with permanent injury or death (Table 22-6). However, all members of the cardiac surgery team must be able to respond to perfusion emergencies to limit the likeli-Ascending aortic cannulas can be malpositioned such that the out ow jet is direct-ed primarily into the innominate artery, the left common carotid artery (rare), or the left subclavian artery (rare). In the rst two circumstances, unilateral cerebral hyperperfu-sion, usually with systemic hypoperfusion, occurs, whereas ow directed to the subclavian artery results in global cerebral hypoperfusion. Despite the fact that not all combinations of arterial pressure monitoring site and cannula malposition produce systemic hypotension, it is commonly regarded as a cardinal sign of cannula malposition. For example, right arm blood pressure monitor and innominate artery cannulation, or left arm monitor and left subclavian artery cannulation may result in high arterial pressure on initiation of bypass. With other positioning and monitoring combinations, investigators report per-sistently low systemic arterial pressure (MAP25 to 35 mmHg), which is poorly respon-sive to increasing pump ow or vasoconstrictors. Over time (minutes), signs of systemic hypoperfusion (e.g., acidemia, oliguria) develop. Because a variable period of systemic hypotension with CPB initiation is nearly always seen with hemodilution, hypotension alone is not signi cant evidence to establish a diagnosis of arterial cannula malposition. On initiation of CPB and periodically thereafter, it is advisable to inspect the face for color change and edema, rhinorrhea, or otorrhea and to palpate the neck with onset of cooling for temperature asymmetry. EEG monitoring has been advocated as a method of detect-ing cannula malposition. Perfusion VEXTRACORPOREAL CIRCULATION538 Two other arterial cannula malpositions are possible: abutment of the cannula tip against the aortic intima, which results in high line pressure, poor perfusion, or even acute dissection when bypass is initiated, and the cannula tip directed caudally toward the aortic valve. This may result in acute aortic insuf ciency, with sud-den left ventricular distention and systemic hypoperfusion on bypass. If the aortic in ow cannula is soft, aortic cross-clamping will occlude the arterial perfu
sion line, which can rupture the aortic in ow line. Suspicion of any cannula malposition must Signs of arterial dissection, often similar to those of cannula malposition, must also be sought continuously, especially on initiation of CPB. Dissection may orig-inate at the cannulation site, aortic cross-clamp site, proximal vein graft anas-tomotic site, or partial occlusion (side-biting) clamp site. Dissections are due to intimal disruption, or more distally to fracture of atherosclerotic plaque. In either case, some systemic arterial blood flow becomes extraluminal, being forced into the arterial wall. The dissection propagates mostly in the direction of the systemic flow but not exclusively. Extraluminal blood compresses the luminal origins (take-offs) of major arterial branches such that vital organs (e.g., heart, brain, kidney, intestinal tract, spinal cord) may become ischemic. Because sys-temic perfusion may be low, and origins of the innominate and subclavian arter-ies may be compressed, probably the best sign of arterial dissection is persistently low systemic arterial pressure. Venous drainage to the pump decreases (blood is sequestered), and arterial inflow “line pressure” is usually inappropriately high. The surgeon may see the dissection if it involves the anterior or lateral ascending Stoney 1972-1977 Wheeldon 1974-1979 IncidentsPI/D IncidentsPI/DIncidentsPI/DAir embolism(2) 1.140.41(2) 0.790.18(6) 0.800.12Coagulopathy(1) 1.260.51(6) 0.260.09(8) 0.210.05Electrical failure(3) 0.670.01(1) 1.000.06(4) 0.840.003(4) 0.380.02(5) 0.270(7) 0.300.007(5) 0.330.02(3) 0.590(3) 0.880.07Hypoperfusion——(4) 0.300.18(2) 0.960.15———(1) 2.800.22Drug error————(5) 0.820.08*The ve most common complications for each study are listed as incidence per 1000 perfusions and the number of permanent injuries and mortalities as incidence per 1000 perfusions. The num-from Stoney WS, Alford WC Jr, Burrus GR, et al: Air embolism and other accidents using pump oxygenators. Ann Thorac Surg 29:336, 1980; Wheeldon DR: Can cardiopulmonary bypass be a safe procedure? In Longmore DB (ed): Towards Safer Cardiac Surgery. Lancaster, London, MTP, 1981, pp and Kurusz M, Conti R, Arens JF, et al: Perfusion accident survey. Proc Am Acad from the Three Perfusion Surveys 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST539 aorta (bluish discoloration), or both. It is possible the surgeon may not see any sign of dissection, because the dissection is out of view (e.g., posterior ascending aorta, aortic arch, descending aorta). Dissection can occur at any time before, during, or after CPB. As with cannula malposition, a suspicion of arterial dissec-tion must be brought to the attention of the surge
on. The anesthesiologist must not assume that something is suddenly wrong with the arterial pressure trans-ducer but should “think dissection.”After a dissection of the ascending aorta is diagnosed, immediate steps to mini-mize propagation must be taken. If it has occurred before CPB, the anesthesiologist should take steps to reduce MAP and the rate of rise of aortic pressure (dP/dt). If it occurs during CPB, pump ow and MAP are reduced to the lowest acceptable levels. Arterial perfusate is frequently cooled to profound levels (14° to 19°C) as rapidly as possible to decrease metabolic demand and protect vital organs. A different arte-rial cannulation site is prepared (e.g., the femoral artery is cannulated or the true aortic lumen is cannulated at a site more distal on the aortic arch). Arterial in ow is shifted to that new site in hopes that perfusing the true aortic lumen will reperfuse vital organs. The ascending aorta is cross-clamped just below the innominate artery, and cardioplegia is administered (into the coronary ostia or coronary sinus). The aorta is opened to expose the site of disruption, which is then resected and replaced. Reimplantation of the coronary arteries or aortic valve replacement, or both, may be necessary. The false lumina at both ends of the aorta are obliterated with Te on buttresses, and the graft is inserted by end-to-end suture. With small dissections it is sometimes possible to avoid open repair by application of a partial occlusion clamp with plication of the dissection and exclusion of the intimal disruption. In some cases of arterial dissection during CPB, TEE has been found useful. Although provisional diagnoses were made on the basis of traditional signs, TEE allowed assessment of the origin and extent of dissection. Diagnosis of arterial dissection has also been Arterial dissections originating from femoral cannulation also necessitate reduc-tions in arterial pressure, systemic ow, and temperature. If the operation is near completion, the heart may be transfused and CPB discontinued; otherwise, the aortic arch must be cannulated and adequate systemic perfusion restored to allow comple-Macroscopic gas embolus is a rare but disastrous CPB complication. Studies in 1980 reported incidences of recognized massive arterial gas embolism of 0.1% to 0.2%. The current incidence is probably lower because of the widespread use of reservoir level alarms and bubble detection devices. Between 20% and 30% of affected patients died immediately, with another 30% having transient or non-debilitating neurologic deficits, or both. Circumstances that most commonly contributed to these events were inattention to oxygenator blood level, reversal of left ventricular vent flow, or
unexpected resumption of cardiac ejection in a previously opened heart.The pathophysiology of cerebral gas embolism (macroscopic and microscopic) is not well understood. Tissue damage after gas embolization is initiated from sim-ple mechanical blockage of blood vessels by bubbles. Although gas emboli may be absorbed or pass through the circulation within 1 to 5 minutes, the local reaction of platelets and proteins to the blood gas interface or endothelial damage is thought to potentiate microvascular stasis, prolonging cerebral ischemia to the point of infarc-tion. Areas of marginal perfusion, such as arterial boundary zones, do not clear gas VEXTRACORPOREAL CIRCULATION540 emboli as rapidly as well-perfused zones, producing patterns of ischemia or infarc-Recommended treatment for massive arterial gas embolism includes immediate cessation of CPB with aspiration of as much gas as possible from the aorta and heart, assumption of steep Trendelenburg position, and clearance of air from the arterial perfusion line. After resumption of CPB, treatment continues with implementation or deepening of hypothermia (18° to 27°C) during completion of theclearance of gas from the coronary circulation before emergence from CPB, and administration of glucocorticoids in an attempt to minimize cerebral edema. In many reports of patients suffering massive arterial gas embolus, seizures occurred postoperatively and were treated with anticonvulsants. Because seizures after ischemic insults are associated with poor outcomes, owing perhaps to hypermetabolic effects, prophylactic phenytoin seems reasonable. Hypotension has been shown to lengthen the residence time of cerebral air emboli and worsen the severity of resulting ischemia. Maintenance of moderate hypertension therefore is reasonable and clini-cally attainable to hasten clearance of emboli from the circulation and, hopefully, Many clinicians have reported dramatic neurologic recovery when hyperbaric therapy is used for arterial gas embolism, even if delayed up to 26 hours after the event. Spontaneous recovery from air emboli has also been reported, and no prospec-tive study of hyperbaric therapy in the cardiac surgery setting has been performed. Few institutions that do cardiac surgery have an appropriately equipped and staffed compression chamber to allow expeditious and safe initiation of hyperbaric therapy. Nonetheless, immediate transfer by air is often possible and should seriously be con-sidered. It seems reasonable to expect that institutions that do cardiac surgery should In 1980, Mills and Ochsner17 suggested venoarterial perfusion as an alternative to hyperbaric therapy. Retrograde perfusion through the SVC cannula at 1.2 L/min at 20°C for 1 to 2 minutes was used in v
e of their eight patients with massive gas embolism. The goal was to ush air from the cerebral arterial circulation. None of the patients so treated had evidence of neurologic injury. Other reports using this technique have followed.Venous Air LockAir entering the venous out ow line can result in complete cessation of ow to the venous reservoir, and this is called air lock. Loss of venous out ow necessitates immediate slowing, even cessation of pump ow, to prevent emptying the reservoir and subsequent delivery of air to the patient’s arterial circulation. After an air lock is recognized, a search for the source of venous out ow line air must be undertaken (e.g., loose atrial purse string, atrial tear, open intravenous access) and repaired In this case, the venous out ow limb of the CPB circuit is incorrectly connected to the arterial in ow cannula and the arterial perfusion limb of the circuit is attached to the venous cannula. On initiation of CPB, blood is removed from the arterial cir-culation and returned to the venous circulation at high pressure. Arterial pressure is found to be extremely low by palpation and arterial pressure monitoring. Very low arterial pressures can also (more commonly) be due to dissection in the arterial tree. In the latter case, the perfusionist will rapidly lose volume, whereas with reversed cannulation, the perfusionist will have an immediate gross excess of volume. If high 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST541 pump ow is established, venous or atrial rupture may occur. The CVP will be dra-Line pressure is the pressure in the arterial limb of the CPB circuit. Because arterial cannulas are much smaller than the aorta, there is always a pressure drop across the aortic cannula. Arterial in ow line pressure will always be considerably higher than systemic (patient) arterial pressure. The magnitude of the pressure drop depends on cannula size and systemic ow; small cannulas and higher ows result in greater gradients. The CPB pump must generate a pressure that overcomes this gradient to provide adequate systemic arterial pressure. For a typical adult (i.e., MAP of about 60 mmHg, systemic ow of about 2.4 L/min/m, and a 24-Fr aortic cannula), line pressure in an uncomplicated case usually ranges from 150 to 250 mmHg. The t-tings on the arterial in ow line are plastic; the ttings and the line itself can rupture. air is found in the arterial circulation, an air embolus protocol is initiated. Once arte-rial air is cleared, the circuit is correctly reconnected and CPB restarted. In adults, the venous out ow limb of the CPB circuit is a larger-diameter tubing than the arterial in ow tubing, precisely
to eliminate reversed cannulation. This is why reversed can-nulation is rare in adults, but it has happened. In pediatric cases, the arterial in ow Care of the Gravid Patient during BypassStudies assessing the effects of cardiac surgery and CPB on obstetric physiology and fetal well-being are lacking. However, several reviews and many case reports describe individual experience in caring for the gravid patient and fetus during cardiac surgery and extracorporeal circulation. These surveys and anecdotal reports, along with an understanding of the well-documented physiology of pregnancy and the effects of cardiac therapeutics on fetal physiology, can serve as a basis for a rational approach The pregnant patient undergoing cardiac surgery requires the usual monitors emloyed during cardiac surgery, as well as monitors that can assess fetal well-being. Monitors that help assess the adequacy of maternal cardiovascular performance and oxygen delivery to the fetus are of paramount importance. Little is known about the effects of cardiovascular drugs and other therapeutic measures on the pregnant cardiac patient undergoing CPB. Appropriate monitors permit the assessment of an Uterine activity should be monitored with a tocodynamometer applied to the maternal abdomen. This monitor transduces the tightening of the abdomen during uterine contractions. As is the case with other types of major surgeries, the tocody-namometer should not interfere with the conduct of cardiac surgery; if necessary, the monitor may be intermittently displaced by the operating surgeon. The use of an intra-amniotic catheter to monitor uterine activity and pressure may be inadvis-able in a patient who will be fully heparinized. Intraoperative uterine contractions may have a deleterious effect on fetal oxygen delivery (by causing an increase in uterine venous pressure and decrease in uterine blood ow) and signal the onset of preterm labor. Use of the tocodynamometer is imperative, because it will provide VEXTRACORPOREAL CIRCULATION542 important information about the state of the uterus and allow intervention if nec-essary. Various reports have documented the common occurrence of uterine con-tractions during cardiac surgery and CPB. Uterine contractions may appear at any time during the perioperative period but occur most frequently immediately after the discontinuation of CPB and in the early ICU period. It is therefore important to leave the tocodynamometer in place after the completion of surgery. Although uterine contractions occur frequently in the perioperative course, they usually are effectively treated with magnesium sulfate, ritodrine, or ethanol infusions, and they do not result in preterm labor and fetal demise.Fetal heart rate (FHR) monit
ors should be employed in all gravid patients after 16 weeks’ gestation, because one of the primary perioperative goals is to avoid fetal loss. Use of an FHR monitor permits recognition of fetal distress and allows the clinician to institute measures to improve fetal oxygen delivery. The FHR monitor recognizes and records the FHR, FHR variability, and uterine contractions. A spinal electrode placed in the fetal scalp gives the most reliable fetal ECG and therefore the best FHR information. However, this method may be undesirable in the presence of maternal anticoagulation. External FHR monitoring, using ultrasound, phonocardiography, The cardiac surgeon and perfusionist may not be familiar with uterine and FHR monitors; the anesthesiologist is accustomed to caring for these patients during labor and delivery and can assess uterine and FHR tracings. However, in some clinical circumstances, such as preoperative fetal distress, or anticipated need for emergency cesarean section during cardiac surgery, having a perinatologist or an obstetrician FHR is usually normal in the pre-bypass period but decreases precipitously with the initiation of CPB and remains below normal for the entire bypass period. There are many potential causes of this observed decrease in FHR. Persistent fetal brady-cardia is a classic sign of acute fetal hypoxia. However, in the CPB setting, especially when hypothermia is employed, it is dif cult to ascribe fetal bradycardia to hypoxia or to decreased fetal oxygen demand. Fetal tachycardia typically occurs after the discontinuation of bypass support. This tachycardia may represent a compensatory mechanism for the oxygen debt incurred during CPB. The FHR usually returns to Interventions optimizing maternal blood oxygen content, correcting any acid-base imbalance, and replenishing fetal glycogen stores may alleviate signs of fetal hypoxia. Some clinicians recommend an increase in CPB pump ow to improve fetal oxygen delivery.The conditions of extracorporeal circulation—nonpulsatile blood ow, hypothermia, anemia, and requisite anticoagulation—will likely have a negative impact on fetal well-being during CPB. There are no studies that recommend a CPB management strategy in gravid patients. Recommendations are summarized (Table 22-7) for the management of bypass in pregnant patients.Optimal CPB blood ow in the gravid patient is unknown. However, the increase in CO associated with pregnancy is well de ned, and it might be argued that high blood ows during CPB are more physiologic in the gravid patient. It has been suggested that ow during CPB in the pregnant patient be maintained at a minimum of 3.0 L/min/mA few reports demonstrate that increasing CPB circuit blo
od ow improves FHR, sug-gesting improvement in fetal oxygen delivery. 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST543 Under normal conditions, uterine blood ow is determined solely by maternal blood pressure, because the placental vasculature is maximally dilated. However, it is not known what factors determine uterine blood ow during the very abnormal condi-tion of CPB. For example, catecholamine levels increase by several times during CPB; therefore, uterine vascular resistance may increase during extracorporeal circulation in response to increased levels of norepinephrine and epinephrine. However, regard-less of the state of uterine vascular resistance during CPB, maternal blood pressure will be an important determinant of uterine blood ow and fetal oxygen delivery. Moderately high pressure (mean arterial pressure 65 mmHg) should be employed TEMPERATUREThere are theoretical advantages and disadvantages for normothermic and hypothermic CPB in the gravid patient. Hypothermia can cause fetal bradycardia and may lead to fetal ventricular arrhythmias resulting in fetal wastage. Rewarm-ingfterhypothermic bypass may precipitate uterine contractions and preterm labor.However, others reported the onset of uterine contractions at the time of discontinuation of bypass support in spite of normothermic perfusion. Uterine VariableRecommended Value/ Blood pressure (MAP)60-70 mmHgOxygenator typeMembraneDuration of perfusionMinimized (?)Pulsatile perfusion? Recommendations for the Conduct of Extracorporeal Circulation in the Gravid Patient VEXTRACORPOREAL CIRCULATION544 contractions also occur at various times in the post-bypass and postoperative periods. The association of uterine contractions with rewarming after hypothermic bypass is unclear.Hypothermia may be protective to the fetus during extracorporeal circulation by decreasing fetal oxygen requirements. Perfusion temperatures of 25° to 37°C have been used in gravid patients undergoing CPB. There are no data that suggest hypo-thermia is harmful to the mother orfetus undergoing bypass. Normothermic CPB may increase the likelihood ofuntoward neurologic sequelae in the mother, an event Cardiopulmonary bypass (CPB) provides extracorporeal maintenance of respi-ration and circulation at hypothermic and normothermic temperatures. CPB permits the surgeon to operate on a quiet, or nonbeating, heart at hypothermic CPB is associated with a number of profound physiologic perturbations. The nervous system, kidneys, gut, and heart are especially vulnerable to isControversy regarding the optimal management of blood ow, pressure, and temperature during CPB remains. Perfusion should be adequate to support ongoing oxygen requirements; mean arterial pressures of
more than 70 mmHg may bene t patients with cerebral and/or diffuse arthrosclerosis. Arterial blood The initiation and termination of CPB are key phases of a cardiac surgery procedure, but the anesthesiologist must remain vigilant throughout the entire bypass.CPB is a complex system that is vulnerable to accidents. Careful and constant among the anesthesiologist, surgeon, perfusionist, and nurse is Minimally invasive cardiac surgery can be performed with port-access bypass circuits. This approach adds considerable complexity to the procedure and is Bloodless cardiac surgery is possible, and numerous approaches including auto-Total CPB can be tailored to produce deep hypothermic, circulatory arrest, or artial bypass. The special techniques require sophisticated monitoring and care. Newman MF, Croughwell ND, White WD, et al: Effect of perfusion pressure on cerebral blood ow Slater JM, Orszulak TA, Cook DJ: Distribution and hierarchy of regional blood ow during hypother- Mora CT, Henson MB, Weintraub WS, et al: The effect of temperature management during cardio-pulmonary bypass on neurological and neuropsychological outcomes in coronary revascularization Stone JG, Young WL, Smith CR, et al: Do standard monitoring sites re ect true brain temperature Kiziltan HT, Baltali M, Bilen A, et al: Comparison of alpha-stat and pH-stat cardiopulmonary bypass in relation to jugular venous oxygen saturation and cerebral glucose-oxygen utilization. Anesth Analg 22CARDIOPULMONARY BYPASS AND THE ANESTHESIOLOGIST545 Russell JA, Navickis RJ, Wilkes MM: Albumin versus crystalloid for pump priming in cardiac surgery: Roach GW, Kanchuger M, Mora Mangano CT, et al: Adverse cerebral outcomes after coronary bypass Mora Mangano CT, Diamondstone LS, Ramsay JG, et al: Renal dysfunction following myocardial revascularization: Risk factors, adverse outcomes and hospital resource utilization. Ann Intern Med RA, Orr RK, Porter D, et al: Gastrointestinal complications following cardiac surgery: An Z, Lockhart CH, Weiner M, Klingensmith G: Advances in diabetic management: Implications TH, Davila-Roman VG, Barzilai B, et al: Management of the severely atherosclerotic ascend-ing aorta during cardiac operations: A strategy for detection and treatment. J Thorac Cardiovasc Surg E, Dhara S: Monitoring oxygenator expiratory iso urane concentrations and the bispectral index to guide iso urane requirements during cardiopulmonary bypass. J Cardiothorac Vasc Anesth CA, Savino JS, Weiss RL: Transesophageal echocardiographic diagnosis of aortic dissection NL, Ochsner JL: Massive air embolism during cardiopulmonary bypass: Causes, prevention, F, Mercogliano D, Cavalletti C, et al: Cardiopulmonary bypass in