
ASSOPROFPEDIATRICS ICHGOVT MEDICAL COLLEGEKOTTAYAM LEARNING OBJECTIVES To write 2 agents causing whoop like cough To list 2 clinical features of whooping cough To name 3 complication of whooping cough ID: 911686
Download Presentation The PPT/PDF document "WHOOPING COUGH DR JAYAPRAKASH. K.P" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






Slide1
WHOOPING COUGH
DR JAYAPRAKASH. K.P
ASSO.PROF.PEDIATRICS
ICH,GOVT MEDICAL COLLEGE,KOTTAYAM
Slide2LEARNING OBJECTIVES
To write 2 agents causing whoop like cough
To list 2 clinical features of whooping cough
To name 3 complication of whooping cough
To suggest 2 preventive measures
Slide3AETIOLOGY
Bordetella pertussis is the cause of epidemic pertussis and the usual cause of sporadic pertussis
Slide4Protracted coughing (which in some cases is paroxysmal) can be caused by Mycoplasma, parainfluenza viruses, influenza viruses, enteroviruses, respiratory syncytial viruses, or adenoviruses.
Slide5PATHOGENESIS
Bordetella organisms are small, fastidious, Gram-negative coccobacilli that colonize only ciliated epithelium. The exact mechanism of disease symptomatology remains unknown
Only B. pertussis expresses pertussis toxin (PT), the major virulence protein.
Slide6filamentous hemagglutinin
, some
agglutinogens
(especially fimbriae [
Fim
] types 2 and 3), and a 69-kDa
nonfimbrial
surface protein
called
pertactin
(Prn)
are important for attachment to ciliated respiratory epithelial cells.
Tracheal
cytotoxin,adenylate
cyclase, and PT appear to inhibit clearance of organisms
Slide7CLINICAL FEATURES
Classically, pertussis is a prolonged disease, divided into
catarrhal,paroxysmal
, and convalescent stages.
The catarrhal stage (1-2
wk
) begins insidiously after an incubation period ranging from 3-12 days with
nondistinctive
symptoms of congestion and
rhinorrhea
variably accompanied by low-grade fever, sneezing, lacrimation, and conjunctival suffusion.
Slide8As initial symptoms wane, coughing marks the onset of the paroxysmal stage (2-6
wk
).
The cough begins as a dry, intermittent,
irritative
hack and evolves into the inexorable paroxysms that are the hallmark of pertussis.
Slide9Posttussive
emesis
is common, and exhaustion is universal. The number
and severity of paroxysms escalate over days to a week and
remain at that plateau for days to weeks.
. As the paroxysmal stage fades into the convalescent stage (≥2
wk
), the number, severity, and duration of episodes diminish.
Slide10Infants younger than 3
mo
of age do not display the classic stages
.
The catarrhal phase lasts only a few days or is unnoticed, and then, after the most insignificant startle from a draft, light, sound, sucking, or stretching, a well-appearing young infant begins to choke, gasp,
gag,and
flail the extremities, with face reddened
Slide11DIAGNOSIS
A clinical case definition
of cough of 14 days
or longer duration with
at least 1 associated symptom of paroxysms, whoop, or
posttussivevomiting
has a sensitivity of 81% and a specificity of 58% for confirmation of pertussis.
Slide12Pertussis should be suspected
in any individual who has a pure or predominant complaint of cough, especially
if the following
featuresare
absent: fever, malaise or myalgia,
exanthem
or
enanthem
, sore throat, hoarseness,
tachypnea
, wheezes, and rales
Slide13TREATMENT
Infants younger than 3
mo
of age with suspected pertussis usually are admitted to hospital, as are many between 3 and 6
mo
of age unless witnessed paroxysms are not severe, as well as are patients of any age
if significant complications occur.
Slide14Assessing the need to provide oxygen, stimulation, or suctioning requires skilled personnel who can watchfully observe an infant’s ability for self-rescue but who will intervene rapidly and expertly when necessary
Slide15An antimicrobial agent always is given when pertussis is suspected or confirmed, primarily to limit the spread of infection and
secondarilyfor
possible clinical benefit. Macrolides are preferred agents and are similar to one another in terms of in vitro activity
Slide16Azithromycin is the preferred
Isolation
Patients with suspected pertussis are placed in isolation with droplet precautions to reduce close respiratory or mucous membrane contact with respiratory secretions.
All healthcare personnel should wear a mask upon entering the room.
Slide17Care of Household and Other Close Contacts
A macrolide agent should be given promptly to all household contacts and other close contacts, such as those in
daycare
, regardless of age, history of immunization, and symptoms
Slide18COMPLICATIONS
The principal complications of pertussis are
apnea
, secondary infections (such as otitis media and pneumonia
Expected pathogens include Staphylococcus aureus, Streptococcus pneumoniae, and bacteria of oropharyngeal flora.
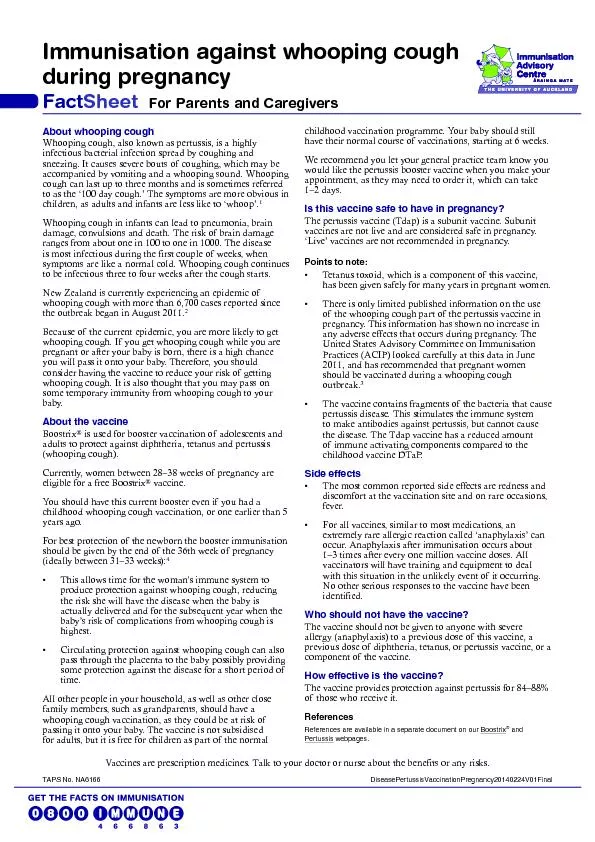
Slide19PREVENTION
Universal immunization of children with pertussis vaccine, beginning in infancy with reinforcing dose(s) through adolescence
Slide20OMP
Slide21