

ember InformationMemberName ember Idon Id CardDate of BirthPhoneMember Address Providingyouris voluntarybut helpfulto accuratelyidentifyyourmedicalsupplying t ID: 893989
Download Pdf The PPT/PDF document "AUTHORIZATION FOR DISCLOSUREPROTECTEDHEA..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.





1 AUTHORIZATION FOR DISCLOSUREPROTECTEDHEA
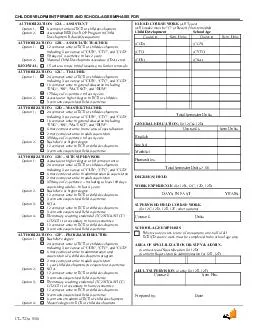
AUTHORIZATION FOR DISCLOSUREPROTECTEDHEALTH INFORMATION ember Information MemberName ember Id(on Id Card) Date of BirthPhone Member Address Providingyouris voluntary,but helpfulto accuratelyidentifyyourmedical supplying the last four digits is also an option InformationbeDisclosed request and authorizeUniversity of Utah Health Plansto DISCLOSEmy protected health information: Pleasecircle indicateyourselection/Full Record OtherPlease indicate: RecipientInformation authorizethefollowingperson(s) or organization to accessmember information: Name:Relationship: Pleaseindicatethepurposethe disclosureof yourmember records: This authorization expires (circle one) One time disclosureOne Year applicable,understandthatbased ontheinformationhavedesignatedabove;thedisclosuremakespursuantthis authorizationmayincludeinformationregardingparticipationin asubstanceabusetreatmentprogram.understandthattheauthorizedrecipientthisinformation SignatureDate Applicable,PrintedNamePersonalRepresentative Descriptionof PersonalRepresentativeAuthority:Parent Power of Attorney (attach documentation)Other (attach documentation) Return completed forms to UUHP Mail: PO Box 45180, SLC UT 84145 Email:uhp@hsc.utah.edu Fax: 801281