
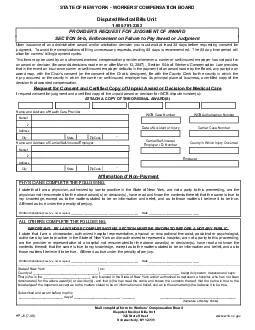
WCB Authorization NumberSTATE OF NEW YORK WORKERS COMPENSATION BOARD18007812362PROVIDERS REQUEST FOR JUDGMENT OF AWARDThisformmaybeusedbyanauthorizedworkerscompensationproviderwheneveracarrierors ID: 883056
Download Pdf The PPT/PDF document "Mail completed form to Workers Compensat..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






1 Mail completed form to: Workers' Compens
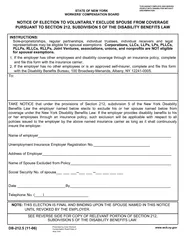
Mail completed form to: Workers' Compensation Board WCB Authorization NumberSTATE OF NEW YORK - WORKERS' COMPENSATION BOARD1-800-781-2362 PROVIDER'S REQUEST FOR JUDGMENT OF AWARD Thisformmaybeusedbyanauthorizedworkers'compensationproviderwheneveracarrierorself-insuredemployerhasnotpaidforanawardordecision(forawards/decisionsmadeonorafterMarch13,2007).Section54-bofWorkers'CompensationLawprovidesthatintheeventaninsurancecarrierorself-insuredemployerdefaultsinthepaymentofanawardmadebytheBoard,anypartytoanawardmay,withtheChair'sconsent(ortheconsentoftheChair'sdesignee),filewiththeCountyClerkforthecountyinwhichtheinjuryoccurredorthecountyinwhichthecarrierorself-insuredemployerhasitsprincipalplaceofbusiness,acertifiedcopyoftheUponissuanceofanadministrativeawardand/orarbitrationdecisionyoumustwaitatleast30daysbeforerequestingconsentforjudgment.Toavoidthecomplicationsoffilingunnecessaryrequests,waiting60daysisrecommended.The60daytimeperiodwill Name and Address of Health Care Provider Address CityStateZip Code- IstatethatIamachiropractor,authorizedhospitalrepresentative,physicaloroccupationaltherapist,podiatristorpsychologist,authorizedbylawtopracticeintheStateofNewYorkand/orauthorizedtorepresentahospital,amnotapartytothisproceeding,amtheproviderorrepresentativeofahospitalnotremuneratedfortheaboveaward(s)ordecision(s),havereadandknowthecontentsthereof;thatthesameistruetomyknowledge,exceptastothemattersstatedtobeoninformationandbelief,andasto IMPORTANT: BY LAW THOSE COMPLETING THIS SECTION MUST BE SWORN TO BEFORE A NOTARY PUBLIC. WCB Case Number Carrier/Self-InsuredEmployer I.D. Number Carrier Case Number Date of Accident or Injury Employer Request for Consent and Certified Copy of Unpaid Award or Decision for Medical CareName and Address of Carrier/Self-Insured Employer That(s)heisthe_________________________,dulylicensedintheStateofNewYorkand/orauthorizedtorepresentahospital,whohasnotbeenremuneratedfortheaboveaward(s)ordecision(s),andthat(s)hehasreadthesameandknowsthecontentsthereof;thatthesameistruetothe Name 1 2 Address Name 1 2 CityStateZip Code- County in Which Injury Occurredwww.wcb. IstatethatIamaphysician,authorizedbylawtopracticeintheStateofNewYork,amnotapartytothisproceeding,amthephysiciannotremuneratedfortheaboveaward(s)ordecision(s),havereadandknowthecontentsthereof;thatthesameistruetomyknowledge,exceptastothemattersstatedtobeoninformationandbelief,andastothosemattersIbelieveittobetrue. PHYSICIANS COMPLETE THE FOLLOWING: Affirmation of Non-Payment ALL OTHERS COMPLETE THE FOLLOWING: Mail completed form to: Workers' Compensation Board WCB Authorization NumberSTATE OF NEW YORK - WORKERS' COMPENSATION BOARD1-800-781-2362 PROVIDER'S REQUEST FOR JUDGMENT OF AWARD Thisformmaybeusedbyanauthorizedworkers'compensationproviderwheneveracarrierorself-insuredemployerhasnotpaidforanawardordecision(forawards/decisionsmadeonorafterMarch13,2007).Section54-bofWorkers'CompensationLawprovidesthatintheeventaninsurancecarrierorself-insuredemployerdefaultsinthepaymentofanawardmadebytheBoard,anypartytoanawardmay,withtheChair'sconsent(ortheconsentoftheChair'sdesignee),filewiththeCountyClerkforthecountyinwhichtheinjuryoccurredorthecountyinwhichthecarrierorself-insuredemployerhasitsprincipalplaceofbusiness,acertifiedcopyoftheUponissuanceofanadministrativeawardand/orarbitrationdecisionyoumustwaitatleast30daysbeforerequestingconsentforjudgment.Toavoidthecomplicationsoffilingunnecessaryrequests,waiting60daysisrecommended.The60daytimeperiodwill Name and Address of Health Care Provider Address CityStateZip Code- IstatethatIamachiropractor,authorizedhospitalrepresentative,physicaloroccupationaltherapist,podiatristorpsychologist,authorizedbylawtopracticeintheStateofNewYorkand/orauthorizedtorepresentahospital,amnotapartytothisproceeding,amtheproviderorrepresentativeofahospitalnotremuneratedfortheaboveaward(s)ordecision(s),havereadandknowthecontentsthereof;thatthesameistruetomyknowledge,exceptastothemattersstatedtobeoninformationandbelief,andasto IMPORTANT: BY LAW THOSE COMPLETING THIS SECTION MUST BE SWORN TO BEFORE A NOTARY PUBLIC. WCB Case Number Carrier/Self-InsuredEmployer I.D. Number Carrier Case Number Date of Accident or Injury Employer Request for Consent and Certified Copy of Unpaid Award or Decision for Medical CareName and Address of Carrier/Self-Insured Employer That(s)heisthe_________________________,dulylicensedintheStateofNewYorkand/orauthorizedtorepresentahospital,whohasnotbeenremuneratedfortheaboveaward(s)ordecision(s),andthat(s)hehasreadthesameandknowsthecontentsthereof;thatthesameistruetothe Name 1 2 Address Name 1 2 CityStateZip Code- County in Which Injury Occurredwww.wcb. IstatethatIamaphysician,authorizedbylawtopracticeintheStateofNewYork,amnotapartytothisproceeding,amthephysiciannotremuneratedfortheaboveaward(s)ordecision(s),havereadandknowthecontentsthereof;thatthesameistruetomyknowledge,exceptastothemattersstatedtobeoninformationandbelief,andastothosemattersIbelieveittobetrue. PHYSICIANS COMPLETE THE FOLLOWING: Affirmation of Non-Payment ALL OTHERS COMPLETE THE FOLLOWING: