
when resting systolic blood pressure exceeds 130 or diastolic blood pressure exceeds 80 mm Hg Even stage 1 hypertension lt14090 has been reported to increase the risk of endorgan damage ID: 1046062
Download Presentation The PPT/PDF document "Antihypertensives Hypertension occurs" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






1. AntihypertensivesHypertension occurs when resting systolic blood pressure exceeds 130 or diastolic blood pressure exceeds 80 mm Hg.Even stage 1 hypertension (<140/90) has been reported to increase the risk of end-organ damage
2. MECHANISMS FOR CONTROLLINGBLOOD PRESSUREArterial blood pressure is directly proportional to cardiac output and peripheral vascular resistanceCardiac output and peripheral resistance are controlled mainly by two overlapping mechanisms: the sympathetic baroreflexes and the renin–angiotensin–aldosterone system Most antihypertensive drugs lower blood pressure by reducing cardiac output and/or decreasing peripheral resistance.
3. A. Baroreceptors and the sympathetic nervous systemA fall in blood pressure causes pressure-sensitive neurons (baroreceptors in the aortic arch and carotid sinuses) to send fewer impulses to cardiovascular centers in the spinal cord. This prompts a reflex response of increased sympathetic and decreased parasympatheticoutput to the heart and vasculature, resulting in vasoconstriction and increased cardiac output.
4. B. Renin–angiotensin–aldosterone systemThe kidney provides long-term control of blood pressure by altering the blood volume Baroreceptors in the kidney respond to reduced arterial pressure (and to sympathetic stimulation of β1-adrenoceptors) by releasing the enzyme renin
5. Renin converts angiotensinogen to angiotensin I, which is converted in turn to angiotensin II, in the presence of angiotensin converting enzyme (ACE). Angiotensin II is a potent circulating vasoconstrictor, constricting both arterioles and veins, resulting in an increase in blood pressure. Angiotensin II stimulates aldosterone secretion, leading to increased renal sodium reabsorption and increased blood volume, which contribute to a further increase in blood pressure
6. Treatment StrategiesGoal for treating HT is: a systolic blood pressure of less than 130 mm Hg and a diastolic BP of less than 80 mm Hg Current recommendations are to initiate therapy with first line (ABCD): ACE inhibitors or angiotensin receptor blocker (ARB), β blockers, calcium channel blocker, and diuretic (thiazide)
7. Compensation for reducing BPespecially in vasodilators Reflex tachycardia & retention of salt & water Unfortunately, the baroreceptor reflex and the renin response are reset to maintain the higher BP. As a result, they respond to a therapeutically lowered BP with compensatory homeostatic responses, which may be significant. These compensatory responses can be counteracted with β blockers and diuretics or angiotensin antagonists.
8. DiureticsA. Thiazide diureticsSuch as hydrochlorothiazide and chlorthalidone lower blood pressure initially by increasing sodium and water excretion. With long-term treatment, plasma volume approaches a normal value, but a hypotensive effect persists that is related to a decrease in peripheral resistance B. Loop diuretics These agents are rarely used alone to treat hypertension, but they are commonly used to manage symptoms of heart failure and edema
9. C. Potassium-sparing diureticsPotassium-sparing diuretics like spironolactone are sometimes used in combination with loop diuretics and thiazides to reduce the amount of potassium loss induced by these diuretics.Spironolactone has an important role in resistant hypertension (3 or more drugs).Main side effect is hyperkalemia
10. β-Adrenoceptor Blocking AgentsThe β-blockers reduce BP primarily by decreasing cardiac output Decrease sympathetic outflow from the central nervous system Inhibit the release of renin from the kidneys, thus decreasing the formation of angiotensin II and the secretion of aldosteroneSelective β1 blockers, such as metoprolol and atenolol are among the most commonly prescribed β-blockers
11. Nebivolol is a selective blocker of β1 receptors, but also increases the production of nitric oxide, leading to vasodilationThe primary therapeutic benefits of β-blockers are seen in hypertensive patients with concomitant heart disease, such as supraventricular tachyarrhythmia, atrial fibrillation, previous myocardial infarction, stable ischemic heart disease, and chronic heart failure. Conditions that discourage the use of β-blockers include asthma, second- and third-degree heart block, and severe peripheral vascular disease
12. ACE InhibitorsACE inhibitors such as captopril , enalapril , and lisinopril Recommended as first-line treatment of hypertension in patients with a variety of compelling indications: Coronary disease or history of diabetes, stroke, heart failure, myocardial infarction, or chronic kidney disease
13. Mechanism of Action ACE inhibitors block the enzyme ACE, which cleaves angiotensin I to form the potent vasoconstrictor angiotensin IIACE is also responsible for the breakdown of bradykinin, a peptide that increases the production of nitric oxide and prostacyclin by the blood vessels. Both nitric oxide and prostacyclin are potent vasodilators. ACEI Bradykinin
14. By reducing circulating angiotensin II levels, ACE inhibitors also decrease the secretion of aldosterone, resulting in decreased sodium and water retention. ACE inhibitors reduce both cardiac preload and after-load, thereby decreasing workload on the heart ACE inhibitors lower blood pressure by reducing peripheral vascular resistance without reflexively increasing cardiac output, heart rate, or contractility
15.
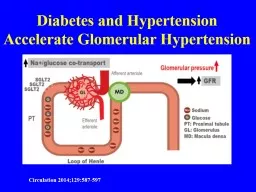
16. Therapeutic usesACE inhibitors are first-line drugs for treating heart failure, chronic kidney disease, and coronary artery disease ACE inhibitors slow the progression of diabetic nephropathy and decrease albuminuria and, thus, have a compelling indication for use in patients with diabetic nephropathy
17. ACE inhibitors are a standard in the care of a patient following a myocardial infarction and first-line in treatment of patients with systolic dysfunction. Chronic treatment with ACE inhibitors achieves sustained blood pressure reduction, regression of left ventricular hypertrophy, and prevention of ventricular remodeling after a myocardial infarction & improve survival
18. PharmacokineticsCaptopril and lisinopril do not undergo hepatic conversion, so may be preferred in patients with severe hepatic impairmentEnalapril is the only drug in this class available intravenously.
19. Adverse effectsDry cough, which occurs in up to 10% of patients, is thought to be due to increased levels of bradykinin and substance P in the pulmonary tree, and it occurs more frequently in women.Angioedema is a rare but potentially life-threatening reaction that may also be due to increased levels of bradykininHyperkalemiaACE inhibitors can induce fetal malformations and should not be used by pregnant women.
20. Angiotensin II Receptor BlockersThe ARBs, such as losartan, block the AT1 receptors, decreasing the activation of AT1 receptors by angiotensin II Their effects are similar to those of ACE inhibitors: arteriolar and venous dilation and block aldosterone secretion, thus lowering blood pressure and decreasing salt and water retention
21. ARBs do not increase bradykinin levelsAdverse effects are similar to those of ACE inhibitors, but risks of cough and angioedema are significantly decreased ARBs should not be combined with an ACE inhibitor for the treatment of hypertension due to similar mechanisms and adverse effects These agents are also teratogenic and should not be used by pregnant women
22. Renin InhibitorA selective renin inhibitor, aliskiren directly inhibits renin and, thus, acts earlier in the renin–angiotensin–aldosterone system than ACE inhibitors or ARBsAliskiren should not be combined with an ACE inhibitor or ARB in the treatment of hypertension Aliskiren can cause diarrhea, especially at higher doses. It also causes cough and angioedema but less often than ACE inhibitors.As with ACE inhibitors and ARBs, aliskiren is contraindicated during pregnancy
23.
24. Calcium Channel BlockersFirst-line treatment option in black patients, and useful in HT with asthma Verapamil mainly on myocardium, amlodipine greatly peripheral. Diltiazem is intermediateHigh doses of short-acting CCB (nifedipine) should be avoided because of increased risk of myocardial infarction due to excessive vasodilation and marked reflex tachycardiaCalcium channel blockers do not dilate veins
25. Verapamil has significant effects on cardiac smooth muscle cells (-ve inotropic) It is also used to treat angina and supraventricular tachyarrhythmias and to prevent migraine and cluster headaches Diltiazem affects both cardiac and vascular smooth muscle cells, but it has a less pronounced negative inotropic effect on the heart compared to that of verapamil.Diltiazem has a favorable side effect profile.
26. Dihydropyridines CCBNifedipine & amlodipine have a much greater affinity for vascular calcium channels than for calcium channels in the heart The dihydropyridines have the advantage in that they show little interaction with other cardiovascular drugs, such as digoxin or warfarin Amlodipine has a very long half-life and does not require a sustained-release formulation.Useful for HT with bronchial asthma/Angina
27. Adverse effects of CCBFirst-degree atrioventricular block and constipation are common dose-dependent side effects of verapamil.Verapamil and diltiazem should be avoided in patients with heart failure or with atrioventricular block due to their negative inotropic (force of cardiac muscle contraction) and velocity of conduction. Dizziness, headache, and a feeling of fatigue caused by a decrease in blood pressure are more frequent with dihydropyridines in addition to constipation.Peripheral edema is another commonly reported side effect of this class. Nifedipine may cause gingival hyperplasia
28. α-ADRENOCEPTOR–BLOCKING AGENTSPrazosin & doxazosin produce a competitive block of α1-adrenoceptors causing relaxation of both arterial and venous smooth muscle. First dose effect ?a-/b-Adrenoceptor blocking Agents Labetalol and carvedilol block α1, β1, and β2 receptors. Carvedilol is indicated in the treatment of heart failure and hypertension. It has been shown to reduce morbidity and mortality associated with heart failure.Labetalol is used in the management of gestational hypertension and hypertensive emergencies
29. Methyldopaα2 agonist that is converted to methylnorepinephrine centrally to diminish adrenergic outflow from the CNSThe most common side effects of methyldopa are sedation and drowsiness. Its use is limited due to adverse effects and the need for multiple daily doses. It is mainly used for management of hypertension in pregnancy, because of safety.
30. VasodilatorsDirect-acting smooth muscle relaxants, such as hydralazine and minoxidilReflexes of increased myocardial contractility, heart rate, and oxygen consumption, prompt angina pectoris, myocardial infarction, or cardiac failure in predisposed individualsVasodilators also increase plasma renin concentration, resulting in sodium and water retention
31. concomitant use of a diuretic (to decrease sodium retention) and a β-blocker (to balance the reflex tachycardia)Hydralazine is an accepted medication for controlling blood pressure in pregnancy-induced hypertension.A lupus-like syndrome can occur with high dosages of hydralazine, but it is reversibleMinoxidil treatment causes hypertrichosis (the growth of body hair). This drug is used topically to treat male pattern baldness
32. Stepped Care (Polypharmacy) Compensatory responses can usually be minimized and toxicity can be reduced by the use of multiple drugs at lower dosages. Drugs are added to a patient’s regimen in stepwise fashion; until adequate blood pressure control has been achieved. The usual steps include (1) lifestyle measures (salt restriction and weight reduction), (2) diuretics (a thiazide), (3) ACE inhibitors or ARBs, (4) a calcium channel blocker or a β blocker or both.
33. MonotherapyIt has been found in large clinical studies that many patients do well on a single drug (eg, a thiazide diuretic, ACE inhibitor, calcium channel blocker, or combined α and β blocker). This approach to the treatment of mild and moderate hypertension has become more popular than stepped care because of its simplicity, better patient compliance, and a relatively low incidence of toxicity.
34. Age and EthnicityOlder patients of most races respond better to diuretics and β blockers than to ACE inhibitors. ACEI for young patients.African Americans of all ages respond better to diuretics and calcium channel blockers, and they respond less well to ACE inhibitors. There is considerable inter-individual variability in metabolism of β blockers.
35. Hypertensive EmergencyHypertensive emergency (formerly malignant HT) is an accelerated severe HT associated with rising blood pressure and rapidly progressing damage to vessels and end organs. Management of hypertensive emergency needs urgent hospitalization. Powerful vasodilators (nitroprusside, or diazoxide) are combined with furosemide and β blockers to lower blood pressure to the (140–160)/(90–110) range promptly (within a few hours). Further reduction is slowly.
36. MCQA 45 year-old man started on therapy for HT and developed persistent dry cough. Which drug is most likely responsible?Lisinopril Losartan Nifedipine Prazosin Propranolol A
37. MCQA 32 year-old woman with HT wishes to become pregnant. Which of the following drugs is absolutely contraindicated in pregnancy?Lapetalol Losartan Methyldopa Nifedipine Hydralazine B
38. MCQWhich of the following correctly ranks from most active on myocardium to most peripherally active?Diltiazem, amlodipine, verapamilVerapamil, diltiazem, amlodipineNifedipine, verapamil, diltiazemAmlodipine, diltiazem, verapamilDiltiazem, verapamil, nifedipine B
39. MCQA 73-year-old man with history of a recent change in his treatment for moderately severe hypertension is brought to the emergency department because of a fall at home. Which of the following drug is most likely to be the cause?Metoprolol Hydrochlorothiazide Lisinopril Prazosin Verapamil D
40. MCQA 58 year old female reports swelling in her feet that began shortly after she started antihyprtensive treatment. Which is most likely to cause peripheral edema? Metoprolol Lisinopril Nifedipine Hydralazine PrazosinC
41. MCQWhich one of the following is characteristic of nifedipine treatment in patients with essential hypertension?(A) Competitively blocks angiotensin II at its receptor(B) Decreases calcium efflux from skeletal muscle(C) Decreases renin concentration in the blood(D) Decreases calcium influx into smooth muscle(E) Increases calcium excretion in the urine D