
Georgetown University MedStar Georgetown University Hospital Georgetown Lombardi Comprehensive Cancer Center Washington DC Catherine M Broome MD Department of Hematology and ID: 1044247
Download Presentation The PPT/PDF document "Faculty Associate Professor of Medicine" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


1.
2. FacultyAssociate Professor of Medicine Georgetown UniversityMedStar Georgetown University HospitalGeorgetown Lombardi Comprehensive Cancer CenterWashington, DCCatherine M.Broome, MDDepartment of Hematology and Stem Cell TransplantUniversity Hospital EssenUniversity of Duisburg-EssenEssen, GermanyAlexanderRöth, MD
3. Learning ObjectivesDescribe the pathogenesis of primary cold agglutinin disease (CAD), the mechanism of disease, its symptoms, and its possible clinical consequences.Diagnose patients suspected of having CAD.Appropriately treat and monitor patients with CAD using non-pharmacologic and pharmacologic options. Describe the mechanism of action, safety and efficacy of new and emerging treatments for CAD.CAD, cold agglutinin disease
4. Module 1Pathogenesis and Clinical Features of Cold Agglutinin Disease
5. Overview of Autoimmune Hemolytic Anemia and CADRare hematologic diseaseCan present acutely in ER or with more chronic symptoms to PCP or other specialistsChallenging at presentation, if clinician is unfamiliar with this rare conditionClinicians need to be aware of pathogenesis, signs, symptoms, and potential risks associated with CAD, along with non-pharmaceutical and pharmaceutical treatment optionsAIHA, autoimmune hemolytic anemia; CAD, Cold Agglutinin Disease.
6. Cold Agglutinin Disease vs Cold Agglutinin Syndrome Primary (idiopathic) Cold Agglutinin Disease (CAD)CAD is a subtype of AIHA caused by IgM autoantibodies, which tend to react at cold temperaturesCAs are IgM antibodies that bind to RBC antigens at less than core body temperatures (37°–39° F | 3°–4° C)Secondary: Cold Agglutinin Syndrome (CAS)Also, an AIHA mediated by IgM autoantibodiesAssociated with systemic disease, most commonly either infection or malignancyOften frequent causes: Mycoplasma pneumoniae pneumonia, Epstein-Barr virus infection, or indolent lymphomaAIHA, autoimmune hemolytic anemia; IgM, Immunoglobulin M; RBC, red blood cells
7. What is Cold Agglutinin Disease?CAD defined: Rare, chronic hemolytic disorder caused by anti–RBC IgM autoantibodies, most often (>90%) monoclonal with k light-chain restriction recognizing the I antigen on the surface of RBCHemolysis in CAD is complement-dependent with mainly extravascular hemolysis [typically in liver]Represents 15% to 25% (~20%) of all AIHAsIt may be exacerbated by many things, including cold temperaturesAIHA, autoimmune hemolytic anemia; IgM immunoglobulin M
8. Prevalence of Patients with CADAffects ~one person per million every year5200 living with CAD in the United StatesAffects middle-aged and elderly people 40–80 years of ageAverage age of onset 60 years of ageMore common in women than menCAD, Cold Agglutinin Disease.
9. Pathogenesis of Cold Agglutinin DiseaseRare form or subtype of AIHA caused by cold-reacting IgM autoantibodiesCharacterized by both:IgM-mediated agglutination of erythrocytes Hemolysis mediated by activation of the classical complement pathway CAs are IgM antibodies that bind to RBC antigens at cooler than core body temperatures (often in extremities)warm-antibody AIHA (wAIHA) cold-antibody AIHA (cAIHA)Hill QA, et al. Blood. 2019;134:4790. AIHA, autoimmune hemolytic anemia; IgM, Immunoglobulin M; RBC, red blood cells.
10. Mechanism of DiseaseAcrocyanosis-agglutination of red blood cells mediated by IgM Berentsen S. Br J Haematol. 2018;181(3):320-330.IgM, Immunoglobulin M.
11. Mechanism of DiseaseBerentsen S. Front Immunol. 2020;11:590.Hemolysis in CAD
12. Complement Cascade in Cold Agglutinin DiseaseRöth et al., N Engl J Med. 2021;384(14):1323-1334.PhagocytosisPathogen LysisIntravascular hemolysisC1 complexC1qC1rC1sExtravascular hemolysisC5 inhibitorEculizumab1 , Ravulizuzmab,Crovalimab Factor B inhibitorIptacopanFactor D inhibitorDanicopan C3 inhibitorPegcetacoplan C1 inhibitorSutimlimabANX005C1-INH
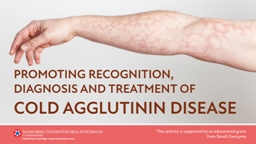
13. Clinical Features of Cold Agglutinin DiseaseHemolysis/Hemolytic anemiaFatigueDyspneaHemoglobinuriaJaundiceAcrocyanosisRaynaud‘s phenomenaLivedo reticularisGangrene1. Berentsen S. Br J Haematol. 2018;181(3):320-330. 2. Röth A, Dührsen U. Eur J Haematol. 2010;84(1):91. 3. Onishi S et al. J Cardiol Cases. 2016;15(2):43-45. 4. Jäger U et al. Blood. 2019 Feb 28; 133(9): 893–901. 5. Kohlert S et al. J Otolaryngol. 2019;48(1):52. 6. Jeskowiak A, George T. N Engl J Med. 2013; 369:e1. 7. Sharma K, Patel A. N Engl J Med. 2019;381:e27.Complement-driven symptoms1-4Cold-induced agglutination (IgM)-driven symptoms5-7
14. Clinical Phenotype of CADTypeDefinitionN%1Hemolytic anemia with circulatory symptoms grade 1 or absent14669.52Hemolytic anemia with circulatory symptoms grade 2–34421.03Circulatory symptoms with compensated hemolysis209.5Berentsen et al. Blood. 2020;136(4):480-488.Circulatory symptoms grade 1, acrocyanosis only; grade 2, Raynaud-like symptoms interfering with daily living; grade 3, gangrene or ulcerations.All patients with available data 210 100.0 CLINICAL PHENOTYPE FREQUENCY
15. Possible Consequences of CAD1. Berentsen S. Br J Haematol. 2018;181:320-330.2. Broome CM, et al. Res Pract Thromb Haemost. 2020;4:628-635.3. Bylsma LC, et al. Blood Adv. 2019;3:2980-2985. 4. Hill QA, et al. Blood. 2019;134:4790. 5. Bylsma LC, et al. Blood Adv. 2019;3:2980-2985. CAD, Cold Agglutinin Disease; TE, thromboembolic events.Transfusions required50% considered transfusion dependent for shorter or longer periods1Elevated thromboembolic threat2,3Increased risk of venous thromboembolism (or other TEs)62% higher incidence of thromboembolic events2Reduced quality of lifeMortality dataHill et al 2019 study in U.S.4Danish Registry, Bylsma et al 20195Patients diagnosed with CAD vs non-CAD, matched population, have higher mortality rate
16. Supportive Care of CADAvoidance of cold temperatures (warm clothing, avoidance of cold drinks, ice-cream, cold air, cold infusions/transfusions etc.)Early and consequent antibiotic treatment of bacterial infections to avoid hemolytic crisisTransfusions (low plasma content, no plasma) when indicated (extremity should be kept warm, in-line blood warmer)Oral supplementation of folic acid (5 mg/d); vitamin B12 or iron (if deficient)Adequate hydration in critical hemolysisThromboprophylaxis with low molecular weight heparin etc. for patients with acute/severe exacerbation of hemolysisGertz. Br J Haematol. 2007;138:422-29; Berentsen et al. Hematology. 2007;12:361-70; Petz. Blood Reviews. 2008;22:1-15; Röth et al. Eur J Haematol. 2010;84:91; Berentsen et al. Hematol Oncol Clin N Am. 2015;29:455-71; Wouters et al. Haemtologica. 2015;100: 1388-95.
17. Management of CADManagement largely unsatisfactory (with no approved treatment)Therapy is mainly directed at the degree of anemiaAvoidance of cold environments (<30º C in exposed skin vessels)Treat underlying disease (if possible)Transfusion of RBCs if necessarySometimes effective emergency treatment neededSteroids, alkylating agents, and splenectomy are not effectiveGertz. Br J Haematol. 2007;138:422-29; Berentsen et al. Hematology. 2007;12:361-70; Petz. Blood Reviews. 2008;22:1-15; Röth et al. Eur J Haematol. 2010;84:91; Berentsen et al. Hematol Oncol Clin N Am. 2015;29:455-71; Wouters et al. Haemtologica. 2015;100: 1388-95. Jäger et al. Blood Rev. 2020 May;41:100648.
18. Mortality Data Among Patients with CAD: Danish Registry 1999–2013Danish National Patient Registry demonstrated significant increase in mortality for CAD patients compared with matched individuals from the general population.First study to compare thromboembolism and mortality risk in CAD against general population.Bylsma LC, et al. Blood Adv. 2019;3:2980-2985.Table adapted from Bylsma LC, et al. 2019 data.Years after Diagnosis/ Cohort Entry CAD CohortMatched comparisons 183.15%96.71%375.67%89.83%560.95%82.11%Mean survival8.5 yearsNot reachedSurvival Probability
19. Mortality Among Patients with CAD: Recent Data from United States StudyHill et al. evaluated mortality risk in largest cohort of CAD patients in the U.S. (vs non-CAD, matched pop)Higher mortality rate in CAD cohortStudy period: January 2007–September 2018651 CAD patients and 3,255 matched non-CAD controls identified35% (n=228) CAD patients and 20% (n=641) non-CAD patients experienced ≥1 TE (P<0.001)Median age 72 years for both cohortsMostly female patients (CAD 64%; non-CAD 65%) Caucasian (CAD 85%; non-CAD 85%)Important to be aware of this dataHill QA, et al. Blood. 2019;134(suppl 1):4790. TE, thromboembolic event.
20. Mortality Among Patients with CAD Hill et al 2019 Data from United States Study cont. Overall mortality rate significantly higher for CAD cohort CAD: 17,512 vs non-CAD: 11,306; P<0.001For patients who experienced ≥1 TE during the study period, mortality rate in CAD cohort was 23,684 vs 15,913 in matched-control cohort (P<0.001)TE, thromboembolic event; SD, standard deviation.Table adapted from Hill QA, et al. Blood. 2019;134(suppl 1):4790.No TE≥1 TECAD cohortMatched non-CAD cohortP-valueCAD cohortMatched non-CAD cohortP-valueMortality rate per 100,000 patients14,184 (n=423)10,176 (n=2,614)<0.00123,684 (n=228)15,913 (n=641)<0.001Mean (SD) age at death, years76 (11) (n=60)82 (9) (n=266)<0.00177 (13) (n=54)82 (7) (n=102)<0.001Mortality Rates and Age at Death in Patients with No or ≥1 TE During the Study Period
21. Module 2Diagnosing Cold Agglutinin Disease
22. Identify Potential PatientsDiagnostic workup of AIHA is essentialTherapeutic management relates specifically to antibody typePatient history and physical examHemoglobin levels and blood cell counts Blood smear examinationDirect antiglobulin test (DAT) Detects immunoglobulin (IGG) and/or complement components on the RBC surface When markers of hemolysis show anemia is hemolytic, DAT is performed to demonstrate autoimmune pathogenesis and identify autoantibodyBarcellini W, et al. Dis Markers. 2015;2015:635670. Jäger U, et al. Blood Rev. 2020;41:100648.AIHA, autoimmune hemolytic anemia; DAT, direct antiglobulin test; RBC, red blood cell.
23. Clinical and Laboratory Characteristics of Patients with CAD (Barcellini et al 2020)Adapted from Barcellini W, et al. J Clin Med. 2020;9:3859. dL, deciliter; Hb, hemoglobin; LDH (ULN), Lactate dehydrogenase expressed as folds of upper limit of normal; Ret, reticulocyte.Median age at diagnosis (Range)Hb (g/dL)Median (Range)LDH (ULN)Median (Range)Ret (x109/L)Median (Range)InadequateReticulocytosisn of pts (%)70 (28–94)8.2 (4.0–13.5)1.4 (0.3–12.2)123 (13–644)69 (64%)
24. Diagnostic Criteria for CADChronic hemolysisPolyspecific DAT positiveMonospecific DAT, strongly positive for C3dCA titer ≥64 at 4°C Bone marrow evaluation—advised in patients with CAD at diagnosisBarcellini W, et al. J Clin Med. 2020;9:3859.Berentsen S. Front Immunol. 2020;11:590.DAT, direct antiglobulin Test.
25. HemoglobinMost Direct Indicator of Clinical SeverityBerentsen S, et al. Blood. 2020;136:480-488.Hb, hemoglobin.Hemoglobin levels Hemoglobin levels Percent in CAD patientsmedian hemoglobin levels of 9.2 g/dL(range: 4.5–15.3 g/dL)mild anemia>10.0 g/dL36% moderate8.0–10.0 g/dL37%severe<8.0 g/dL27%
26. Hemolytic Disease MarkersBarcellini W, et al. Dis Markers. 2015;2015:635670.Diagnostic flowchart for hemolytic diseases. If flowchart turns negative for congenital hemolytic anemia, reconsider acquired causes and vice versa. AIHA: autoimmune hemolytic anemia; CDA: congenital dyserythropoietic anemia; DHTR: delayed hemolytic transfusion reactions; PNH: paroxysmal nocturnal hemoglobinuria; RBC: red blood cells.
27. Recognize Hemolytic BiomarkersBarcellini W, et al. Dis Markers. 2015;2015:635670. Barcellini W, et al. J Clin Med. 2020;9:3859. Berentsen S. Front Immunol. 2020;11:590. CAD, Cold Agglutinin Disease; LDH, Lactate dehydrogenase.Hemoglobin (Hb) (reduced in patients with CAD)Most direct indicator of clinical severityMedian hemoglobin levels of 9.2 g/dL (range: 4.5–15.3 g/dL)Reticulocytes (increased)Indicator of [efficient] bone marrow compensationShould be converted to absolute count, and refer to Hb/hematocrit valuesExpressed as a %Reticulocytopenia may represent medical emergency, may be long-lasting despite therapy, and requires transfusionLDH levels (elevated)Marker of intravascular hemolysisMedian range 1.4 (for patients with CAD)Bilirubin levels (elevated)Catabolism of the protoporphyrin IX ring of hemeGood marker for extravascular and intravascular hemolysis Possible presence of an associated liver disease or concomitant Gilbert syndromeHaptoglobin (reduced)Most sensitive marker; last to be normalized after remission Scavenger of free hemoglobinIncreases during inflammation, nephrotic syndrome, or smoking; Can mask underlying hemolysisFerritin (increased) Indirect marker of the total body amount of iron
28. Module 3Current Treatment Approaches for Patients with Cold Agglutinin Disease
29. Treatment GoalsImprove anemia by increasing Hb levelsAvoid transfusion Improve circulatory symptoms caused by cold temperaturesReduce inflammatory symptomsHb, hemoglobin
30. Supportive Care of CADAvoidance of cold temperatures (warm clothing, avoidance of cold drinks, ice-cream, cold air, cold infusions/transfusions etc.)Early and consequent antibiotic treatment of bacterial infections to avoid hemolytic crisisTransfusions (low plasma content, no plasma) when indicated (extremity should be kept warm, in-line blood warmer)Oral supplementation of folic acid (5 mg/d); vitamin B12 or iron (if deficient)Adequate hydration in critical hemolysisThromboprophylaxis with low molecular weight heparin etc. for patients with acute/severe exacerbation of hemolysisGertz. Br J Haematol. 2007;138:422-29; Berentsen et al. Hematology. 2007;12:361-70; Petz. Blood Reviews. 2008;22:1-15; Röth et al. Eur J Haematol. 2010;84:91; Berentsen et al. Hematol Oncol Clin N Am. 2015;29:455-71; Wouters et al. Haemtologica. 2015;100: 1388-95.
31. Non-Pharma Treatment OptionsNon-pharma treatment options for mild forms of CADThermal protection and cold avoidanceSome patients, avoid cold food and beveragesTransfusions (avoid cold transfusions)Special recommendations Corticosteroids should not be used to treat CADCAD, Cold Agglutinin Disease.
32. Pharmaceutical RecommendationsAvoid corticosteroids Commonly used in wAIHASteroids are ineffective in CADRelatively low efficacy in monotherapy treatment Consider patients for clinical trials for emerging optionsCAD, Cold Agglutinin Disease; wAIHA, warm autoimmune hemolytic anemia.
33. First-Line Treatment StrategyRituximab monotherapy (375 mg/m2 weekly x 4) in frail, multimorbid patientsResponse rate, only 50% effectivePartial responses, almost exclusivelyMedian duration, 12 monthsRituximab-Bendamustine combination therapy (90 mg/m2 day 1,2) Relatively fit patients, severely affected 4 cyclesTrial results yielded 78% response rate, 53% complete response, response duration >88 monthsCan cause neutropenia, with increased chance of adverse eventsRossi G, et al. Blood. 2018;132:547–550. Berentsen et al., Blood, 2017; 130:537-541. Berentsen et al., Blood, 2020; 136:480-488.
34. Combination Therapy—Increases Response RateRituximab-BendamustineBerentsen et al. (n=232) Norway v Italy study showedImprovement up to 78% (from 71%)Complete response 53% (from 40%)Response duration 88 months (7.3 yrs)Limitations≥25% will not respondPatients continue to hemolyzeAwareness of SAEsRisk of neutropeniaInfections may increaseBerentsen S, et al. Blood. 2020;136:480-488. SAEs, serious adverse events
35. Second-Line Treatment StrategyRituximab-Fludarabine (oral, 40 mg/m2)1–3For fit patients (not too young) 40 mg/m2 on days 1–5 Higher response rate ~76% cases Sustained remissionsHigher risk of long-term AEsBortezomib monotherapy (approved for MM and MCL w/at least 1 prior therapy)4,5One cycleEffective in one-third of patients1. Barcellini W, et al. J Clin Med. 2020;9:3859; 2. Berentsen S. Br J Haematol. 2018;181:320-330; 3. Berentsen S. Front Immunol. 202o;11:590; 4. Rossi G, et al. Blood. 2018;132:547–550; 5. Highlights of prescribing information (bortezomib). Accessdata.FDA.gov. Issued June 2008.MCL, mantle cell lymphoma; MM, multiple myeloma.
36. Common Adverse EventsNeutropenia can result in…InfectionConcerns of long-term toxicities Specifically with use of cytostatic agents, fludarabine and bendamustineRituximab infusion reactions, at start
37. Cold Agglutinin Mediated AIHAJäger et al. Blood Rev. 2020 May;41:100648. Röth. Blood. 2020 Jul 23;136(4):380-381.W & W: watch and wait; CAD: Cold Agglutintin Disease; CAS: Cold Agglutinin SyndromePrimary CADCold agglutinin mediated AIHAW & W AsymptomaticRituximab + BendamustineNo Response/RelapseClinical Trial / Experimental TreatmentSutimlimab, BIVV020, Ibrutinib, VenetoclaxSecondary CASTreat underlying disease(if possible)SupportiveCare/Therapy Rituximab + Fludarabine or Bortezomib mono RelapseSymptomatic (anemia, transfusion, circulatory symptoms)Rituximab(375 mg/m2 weekly x 4)(+ Bendamustine for fit patients)Clinical Trial (if available) Emergency Situation EculizumabPlasmapheresisSupportiveCare/Therapy
38. Module 4Emerging Treatments for Cold Agglutinin Disease
39. Unmet Medical NeedHigh frequency of persistent anemia/hemolysisImmunochemotherapy is unsuccessful in at least 25% because of treatment failure or toxicitySmall B-cell clone with low proliferation activity and difficult to target efficientlyNeed for rapid acting therapy, especially in specific clinical settings: acute and severe exacerbations due to infections, major surgery, trauma, cardiac surgeryGertz. Br J Haematol. 2007;138:422-29; Berentsen et al. Hematology. 2007;12:361-70; Petz. Blood Reviews. 2008;22:1-15; Röth et al. Eur J Haematol. 2010;84:91; Berentsen et al. Hematol Oncol Clin N Am. 2015;29:455-71; Wouters et al. Haemtologica. 2015;100: 1388-95.
40. Global Collaborative Efforts for Evidence-Based Treatment1–52017 First International Consensus Meeting1Berentsen et al. Norway v Northern Italy study largest study of patients with verified CAD (n=232) 3Bylsma et al. in Danish study showed CAD patients had increased increased risk of TEs and increased mortality compared with the general population cohort4 Natsuaki et al. in Japanese study showed risk of thrombotic and bleeding events51. Jäger U, et al. Blood Rev. 2020;41:100648; 2. Berentsen S. Br J Haematol. 2018;181:320-330; 3. Berentsen S, et al. Blood. 2020;136:480-488; 4. Bylsma LC, et al. Blood Adv. 2019;3:2980-2985; 5. Natsuaki M, et al. J Am Heart Assoc. 2018;7:e008708. CR, complete response; TE, thromboembolic event.
41. Group of international experts representing study groups, registries, and centers with large scientific and clinical experience met in Vienna (2017)Addressing issues that include no licensed treatment for AIHAs currentlyNew treatment approaches are underway to target underlying mechanisms of hemolysisGoals from 2017 meeting:Improve global level of trainingImprove management Provide basis for clinical trial planningEstablished need for international AIHA networkJäger U, et al. Blood Rev. 2020;41:100648.AIHA, autoimmune hemolytic anemia.
42. Norway v Northern Italy studyLargest study (n=232) of patients with CAD: 24 centers, 5 countries 4-fold differences in prevalence cold vs warmer climates Long-term treatment outcomesRituximab-bendamustine therapy: 78% response rate53% achieved CRResponse duration >88 months; low risk of late malignancies77% est. 5-year sustained remissionRituximab-fludarabine showed higher risk of long-term adverse effects Berentsen S, et al. Blood. 2020;136:480-488.CR, complete response; TE, thromboembolic event.
43. Based on Danish National Patient Registries; Study period: 1999–2013 Examined risk of TEs and mortality in CAD patientsCAD patients had increased mortality compared with the general population cohort Risk of TEs was higher in the CAD patientMedian survival: 8.5 yearsBylsma LC, et al. Blood Adv. 2019;3:2980-2985TE, thromboembolic events.Patients diagnosed with CADMatched controlsN=72720TEs at 1 year7.2%1.9%at 3 years9.0%5.3%at 5 years11.5%7.8%Mortality rates 1 and 5 yrs after diagnosis17% and 39%3% and 18%
44. Status of Potential TargetsPotential targets are based on better understanding of pathogenesis Few therapies for symptomatic CAD patientsNo FDA-approved treatments at this timeSeveral emerging agents are in ongoing clinical trialsJäger U, et al. Blood Rev. 2020;41:100648. Barcellini W, et al. J Clin Med. 2020;9:3859. Broome CM, et al. Res Pract Thromb Haemost. 2020;4:628-635.CAD, Cold Agglutinin Disease.
45. Emerging Treatments (as of June 2021)1. Röth A, et al. Blood Adv. 2018;2:2543-2549.2. Rossi G, et al. Blood. 2018;132:547–550.GIMEMA, Gruppo Italiano Malattie EMatologiche dell'Adulto; Hb, hemoglobin; IV, intravenous; LDH, Lactate dehydrogenase, MoA, mechanism of action.AgentMoAStudy & StatusNTreatment CoursePrimary End PointStudy ResultsEculizumab1C5a and C5b inhibitor DECADE, Phase 2 (NCT01303952)Completed2011–201713600 mg IV infusion qw 4 wks, followed 1 wk later 900 mg thru wk 26Difference in LDH from baseline to last day of therapy (26 wks)Effective reducing transfusion requirementBortezomib226S proteasome inhibitorGIMEMA study Phase 2 (NCT01696474)Completed2012—201721Single course of 1.3 mg/m2 IV on days 1, 4, 8, 11.Achieve transfusion independenceOr significant rise (>20 g/L) of Hb Short course effective in 1/3 patients failing previous treatment
46. Emerging Treatments (as of June 2021) cont.1. Röth A, et al. Blood. 2019; 134:LBA-2.2. Röth A, et al. N Engl J Med. 2021;384(14):1323-1334.3. CADENZA Trial. https://clinicaltrials.gov/ct2/show/NCT03347422.4. Abdullah A. https://coldagglutininnews.com. Posted Dec 11, 2020.EOT; end of treatment; Hb, hemoglobin; MoA, mechanism of action.*FDA Issues CRL regarding the Biologics License Application for Sutimlimab. Nov 2020. AgentMoAStudy & StatusNPrimary End PointStudy ResultsSutimlimab1,2*(BIVV009) C1s inhibitor CARDINAL TrialPhase 3 (NCT03347396)Active, not recruiting 2017– Last updateMarch 2021 24% participants w/response; transfusion independence wk 5–26 (EOT) Hemolysis halted; increased Hb, reduced bilirubin, and reduced fatigueSutimlimab3,4(BIVV009) C1s inhibitor CADENZA Trial, Phase 3 (NCT03347422) Active, not recruiting2017—Est end date Dec 202140% participants w/response; transfusion independence wk 5—26 (EOT) Top-line results expected by the end of 2021.
47. Emerging Treatments (as of June 2021) cont.Ray F. ColdAgglutininNews.com. Posted Nov 2020.ClinicalTrial.gov. Available at https://clinicaltrials.gov/ct2/show/NCT04802057. ClinicalTrial.gov. Available at https://clinicaltrials.gov/ct2/show/NCT04269551.Hb, hemoglobin; IV, Intravenous; MoA, mechanism of action; SC, subcutaneous.AgentMoAStudy & StatusNTreatment CoursePrimary End PointPegcetacoplan (APL-2)1C3/C3b inhibitorPLAUDIT study Ongoing Phase 2 (NCT03226678)Active, not recruiting2017–Est end July 2022 24270mg or 360mg SC daily up to 12 monthsAssessing safety, tolerability, efficacy, and pharmacokinetics of multiple doses SC APL-2Interim data show mean Hb 11.2 g/dL, mean ARC of 64 X 10⁹/L, mean bilirubin 0.4 mg/dL, and mean LDH of 183 U/L BIVV020C1s inhibitor olipudase alfaPhase 1 (NCT04802057)Active/recruiting2021—Est. end 2023 Est. 18multiple IV dosesAssess long-term safety and tolerability in patients with CAD after multiple doses of BIVV020Phase 1b (NCT04269551)Active/recruiting2021—Est. end 2023 Assess long-term safety and tolerability in patients with CAD after a single dose of IV BIVV020single dose of IV BIVV020
48. Eculizumab in CADTherapy-related changes in lactate dehydrogenase levelsRöth A et al. Blood Adv. 2018;2:2543-2549
49. Eculizumab in CADRöth A et al. Blood Adv. 2018;2:2543-2549.Relationship between lactate dehydrogenase response, eculizumab serum levels, and the thermal amplitude of the cold agglutinin. Eculizumab response in a patient with an acute CAS. Urine of patient 5 with severe intravascular hemolysis and hemoglobinuria immediately before (A) and 24 hours after (B) the first dose of eculizumab.
50. Sutimlimab Selectively Targets Complement C1s, Inhibiting Classical Complement Pathway ActivationRöth A, et al. N Engl J Med. 2021;384(14):1323-1334. C1 complexC1qC1rC1sSutimlimabSutimlimab bindsC1sIntravascular hemolysisPathogen LysisExtravascular hemolysisSutimlimab (formerly BIVV009)Humanized monoclonal AbIgG4 (S241P; L248E)Inhibits classical complementLectin and Alternativepathways remain intact
51. CARDINAL: An Open-label, Multicenter Phase 3 Study of Sutimlimab in Patients With Primary Cold Agglutinin Disease Who Have Had a Recent History of Blood TransfusionKey Eligibility CriteriaBaseline HB ≤10 g/dLActive hemolysis: Total bilirubin above normal≥1 blood transfusion w/in 6 months of enrollmentSecondary form, CAS excludedNo treatment with rituximab w/in 3 mos or combo therapies w/in 6 mosDosing:IV, weight-based dosing at Day 0,7, and then every 2 wks<75kg: 6.5g or ≥75kg: 7.5gPrimary Endpoint—Composite Responder Analysis (at TAT)Increase in Hb of ≥2 g/dL from baseline OR normalization to ≥12 g/dL ANDAbsence of transfusion from wks 5 to 26 ANDNo use of protocol prohibited CAD medicationsSecondary Endpoint—Mean change from baseline in Anemia (Hb)Hemolysis (e.g., total bilirubin, LDH)QoL (fatigue, measured by FACIT-F)Transfusions use after the first 5 wksCAS, cold agglutinin syndrome; Hb, hemoglobin; LDH, Lactate dehydrogenase; TAT; treatment assessment time point; QoL, quality of life.Röth A. presented at Late-breaking abstract "Inhibition of Complement C1s with Sutimlimab in Patients with Cold Agglutinin Disease (CAD): Results from the Phase 3 Cardinal Study" at 61st American Society of Hematology Annual Meeting, Dec 2019. Orlando, FL.Röth A, et al. N Engl J Med. 2021;384(14):1323-1334.
52. CARDINAL Trial (Phase 3) Sutimlimab in CADA Phase 3, Pivotal, Open-label, Multicenter Study to Assess the Efficacy and Safety of Sutimlimab in Patients With Primary Cold Agglutinin Disease Who Have a Recent History of Blood TransfusionPresented at Late-Breaking Abstracts Session, ASH, Dec 2019Röth A. presented at Late-breaking abstract "Inhibition of Complement C1s with Sutimlimab in Patients with Cold Agglutinin Disease (CAD): Results from the Phase 3 Cardinal Study" at 61st American Society of Hematology Annual Meeting, Dec 2019. Orlando, FL.Röth A, et al. N Engl J Med. 2021;384(14):1323-1334.ASH, American Society of Hematology; Hb, hemoglobin.Patient Demographics and Disease Characteristics N (%)Mean (range)Patients24Mean age71 (55–85)Female15 (62.5) Mean (range) transfusions in the prior 6 months3.2 (1–19)Patients with ≥1 prior targeted therapy within the last 5 years15 (62.5)Baseline Hb8.6 g/dL (4.9–11.1)
53. CARDINAL Trial ResultsStudy Results (n=24); no placebo arm:Mean Hb level >11 g/dL maintained from wk 3 thru end of studyMean bilirubin levels normalized by week 3 71% did not receive transfusion from wk 5 to wk 26Clinically meaningful reductions in fatigue observed by wk 1 and maintained throughout study92% (22) had at least 1 AE29% (7) had at least 1 SAE, not related to agent No TEs experiencedNo meningococcal infectionsRöth A. presented at Late-breaking abstract "Inhibition of Complement C1s with Sutimlimab in Patients with Cold Agglutinin Disease (CAD): Results from the Phase 3 Cardinal Study" at 61st American Society of Hematology Annual Meeting, Dec 2019. Orlando, FL.Röth A, et al. N Engl J Med. 2021;384(14):1323-1334.AE, adverse event; Hb, hemoglobin; SAE, serious adverse event; TE, thromboembolic event.
54. CARDINAL Trial Summary AnalysisSutimlimab is first-in-class selective inhibitor of the classical complement pathwaySutimlimab demonstrated rapid and sustained efficacy in CADTreatment with sutimlimab prevented hemolysis, significantly increased Hb, and improved QoL (FACIT-F)Targeting C1s in the classical complement pathway represents a novel therapeutic approach for the management of CADSutimlimab has the potential to change treatment practices for patients with CADRöth A. presented at Late-breaking abstract "Inhibition of Complement C1s with Sutimlimab in Patients with Cold Agglutinin Disease (CAD): Results from the Phase 3 Cardinal Study" at 61st American Society of Hematology Annual Meeting, Dec 2019. Orlando, FL.Röth A, et al. N Engl J Med. 2021;384(14):1323-1334.FACIT-F, The Functional Assessment of Chronic Illness Therapy—Fatigue; Hb, hemoglobin; QoL, quality of life.
55. CADENZA Trial (Phase 3) Sutimlimab in CADA Phase 3, Randomized, Double-blind, Placebo-controlled Study to Assess the Efficacy and Safety of Sutimlimab in Patients With Primary Cold Agglutinin Disease Without a Recent History of Blood TransfusionDuration per patient is approximately 1.5 to 2.5 yearsOngoing study; Top-line results expected by the end of 2021.Primary Endpoint: Number of patients responding to treatment with ≥1.5-point increase in Hb levels above baseline, preventing blood transfusion btwn wks 5 and 26 post-treatmentPart A: sutimlimab or placeboParticipant considered responder if they did not receive a blood transfusion from Week 5—26 (EOT) and did not receive treatment for CAD beyond what is permitted per protocolPart B: Response Extension Phase (sutimlimab) solution for IV injection routeNumber of participants with treatment-emergent AEs and SAEsAEs, adverse events; IV, intravenous; SAE, serious adverse event.
56. Common Secondary Outcome MeasuresTransfusion avoidance PRBC units transfused Change in Hb levels Haptoglobin Hemopexin Free hemoglobin Reticulocytes SF-36v2®QLQFACIT-F scale version 4 Six-minute walk test Circulatory symptoms Thrombosis recordFACIT-F, The Functional Assessment of Chronic Illness Therapy – Fatigue; Hb, hemoglobin; PRBC, Packed red blood cell; Quality of Life QuestionnaireClinicalTrials.gov, Cold Agglutinin DiseaseTime frame for measures: baseline to 26 weeks
57. Daratumumab Single-Case StudyDaratumumab targets CD38-positive cells, expressed on plasma cells and lymphoplasmocytesShows immunomodulatory influence on cytokines (IL-6, IL-10, IL-17, IFN-γ, TNF-α, TGF-β)Patient had long history of multi treated CAD (rituximab was ineffective) with severe transfusion-dependent anemia, low cold agglutinin titer, and IgG monoclonal gammopathyCase indicates effectiveness ameliorating anemia and improving disabling circulatory symptoms Although, patient did not experience a complete responseHb levels increased 3 g/dL resulting in transfusion independence Disabling circulatory symptoms disappearedPotential additional therapeutic option for the refractory disease.Zaninoni A, et al. Front Immunol. 2021;12:649441.
58. CADENCE RegistryCold Agglutinin Disease Real World EvidENCE RegistryGlobal Patient Registry will provide perspective longitudinal dataLaunched 2019 to advance understanding of:Patient demographicsClinical presentation and characteristicsCo-morbidities and disease burdenPatterns and use of CAD treatmentsLong-term clinical outcomesPatients’ health-related quality of lifeDifferent geographic locationsRegister your patient | https://coldagglutininnews.com/2021/01/07/cadence-registryAvailable at https://coldagglutininnews.com/2021/01/07/cadence-registrySupported by Sanofi Genzyme
59. In the news, May 2021 (Spain)Note:Patients on anti-compliment agent affecting B-cell function may not be as prone to these exacerbationsMore than symptomatic management for CAD patientsPérez-Lamas L, et al. Am J Hematol. 2021. doi: 10.1002/ajh.26214. epub ahead of print.
60. Module 5Interactive Case Scenario
61. Interactive Patient Case (Dec 2010–June 2013)…December 2010: 62-yo female began feeling fatigue and SOB. Saw PCP with no diagnosis. A few months later was referred to cardiologist with no cardiac pathology detected. Was seen by pulmonary a few months later with no pathology detected. Finally, Jan 2012 noted to be anemic and work up revealed CADTreated Feb 2012 with rituximab 375mg/m2 weekly x 4 weeks and STEROIDS By May 2012 she had a partial responseMay 2012 to June 2013, weaning off steroidsSOB, shortness of breath.
62. Patient Case (June 2013–Jan 2017) continuedJune 2013: Worsening fatigue, SOB, recurrent hemolysisAgain, placed HIGH-DOSE STEROIDS and rituximab 375mg/m2 x 4Steroids tapered off by Jan 2014October 2014 recurrent hemolysis, SOB, fatigue again Placed on STEROIDS; no benefit; again, treated rituximab 375mg/m2 x 4Stable until Dec 2016, then, fatigue and SOB worseJanuary 2017: 4th round of rituximab—no benefitSOB, shortness of breath
63. Patient Case (April 2017) continuedApril 2017: presented to GT with anemia, SOB, lesion on ear and thumbFound to have PULMONARY EMBOLUSStarted on plasma exchangePlasma exchange 2x week plus cyclophosphamide ~one year with Hgb 9, persistent fatigueSOB, shortness of breath
64. Patient Case QuestionWhat should the duration of the anticoagulation be for this patient?3 months6 monthsUntil hemolysis has resolvedIndefinite
65. Patient Case Answer and ExplanationWhat should the duration of the anticoagulation be for this patient?Correct answer is D: IndefiniteExplanation: Patients with CAD remain at risk for venous and arterial thrombotic events even when hemolysis appears inactive. This is believed to be related to chronic complement activation.
66. TakeawaysDiagnostic markers include reduced Hb levels, increased reticulocytes, elevated LDH, elevated bilirubin levels, and reduced haptoglobin.Novel therapeutic approaches on the cusp of approval for the management of CAD.Clinicians should discuss potential clinical trials with patients who fail at first and second-line therapy.Discuss CADENCE Registry and register your patients.Be aware of investigational therapies in pipeline.https://coldagglutininnews.com/2021/01/07/cadence-registryHb, hemoglobin; LDH, LDH, Lactate dehydrogenase.