
Courses in Therapeutics and Disease State Management Epidemiology Common benign neoplasm that affects the majority of elderly mean BPH occurs in approximately 60 of men over 60 years of age and 78 of men over at age 80 ID: 1034280
Download Presentation The PPT/PDF document "Endocrinology: Benign Prostatic Hyperpl..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.






1. Endocrinology: Benign Prostatic HyperplasiaCourses in Therapeutics and Disease State Management
2. EpidemiologyCommon benign neoplasm that affects the majority of elderly meanBPH occurs in approximately 60% of men over 60 years of age and 78% of men over at age 80. Peak incidence of BPH occurs between ages 63 and 65
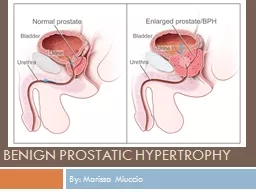
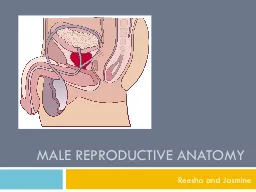
3. Anatomy ReviewLink: Representation of the anatomy of and α-adrenergic receptor distribution in the prostate, urethra, and bladder.Normal prostate in an adult male is 15-20 grams (size of a walnut)
4. PathophysiologyStimulation of the concentrated α1-adrenergic receptors in the prostate causes smooth-muscle contractionResults in compression of the urethra, reduction of the urethral lumen, and decreased urinary bladder emptyingAnatomic enlargement of the gland itself physically blocks the bladder neckLink: Table covering Medical Treatment Options for Benign Prostatic Hyperplasia
5. SymptomsObstructiveDecreased force of streamWeak flowHesitancyStrainingDribblingProlonged voidingIncomplete voidingRetentionIrritativeUrgencyFrequencyNocturiaDysuriaSmall volumeIncontinence
6. ComplicationsAcute urinary retentionUrinary tract infectionsRenal impairment/Renal FailureHematuria when tissue growth exceeds its blood supplyOverflow urinary incontinence
7. Diagnosis and ClassificationAmerican Urological Association Prostate Symptom ScoreNot at all = 0Less than 1 time in 5 = 1 Less than half the time = 2About half the time = 3More than half the time = 4Almost always = 5Over the past month, How often have you had the sensation of not emptying your bladders completely?How often have you had to urinate again in less than 2 hours? How often have you stopped and started when urinating? How often have you found it difficult to postpone urinating ?How often have you had a weak urinary stream?How often have you had to push or strain to begin urinating? How many times did you most typically get up to urinate from the time you went to bed until the time you got up in the morning? None = 0 | Once = 1 | Twice = 2 | 3 times = 3 | 4 times = 4 | 5 times or more = 5Score Mild BPH = 1 to 7 | Moderate = 8 to 19 | Severe = 20 to 35Digital rectal examProstate Specific Antigen (PSA)UrinalysisBUN/CrPost Void ResidualsUrinary flow ratesMedication history
8. Treatment ApproachesGoal is to reduce symptoms and prevent complicationsLink: Comparison Table of α1-Adrenergic Antagonists, 5α-Reductase Inhibitors, Phosphodiesterase Inhibitors, and Anticholinergic Agents for Benign Prostatic Hyperplasia
9. Non-PharmacologicWatchful waitingLifestyle changes in all patientsAvoid medications which contribute to or exacerbate symptomsTestosterone replacementAdrenergic agonists (decongestants)AnticholinergicsDiureticsFluid restriction at bedtimeAvoid caffeine and alcoholScheduled toileting
10. Complementary and Alternative MedicineSaw PalmettoRandomized placebo controlled trials have not demonstrated efficacyLycopeneContradictory studiesCounsel patients to maintain vegetable rich dietPhytosterolsPromising, but not conclusiveDiet rich in vegetables, nuts and legumes
11. Management Algorithm for Benign Prostatic Hyperplasia (BPH)
12. First Line Therapy: Alpha 1 BlockersRelax prostatic smooth muscle tissue, bladder neck, and urethraEqually efficacious within a few daysAll are metabolized by CYP 450 3A4Selection of agent based on age, side effect profile, and cost
13. Alpha 1 BlockersDoxazosinTerazosinTamsulosinAlfuzosinSilodosinBrand NameCardura®Hytrin®Flomax®Uroxatrol®Rapaflo®UroselectiveNoNoYesYesYesDosing2mg titrate to 8mg, XL start at 4mg5mg titrate to 10mg0.4mg (can try 0.8mg)10mg QD8mg (renal dose 4mg)TimingBedtimeBedtimeAfter meals*After mealsAfter meals*Hypotension++++-++Ejaculation Disorders+++++++++++Rhinitis+++++Floppy iris syndrome+
14. 5-Alpha Reductase InhibitorsShrinks enlarged prostate by blocking conversion of testosterone to dihydrotestosterone Equally efficacious, but require at least 6 months of therapyEffectiveness has been best demonstrated in men with significantly enlarged prostates (>40 grams)
15. 5-Alpha Reductase InhibitorsFinasterideDutasterideBrand NameProscar®Avodart®Dosing5mg QD0.5mg QDDecreased Libido++Erectile Dysfunction++Gynecomastia++Cost/day$0.87$3.93Pregnant women should avoid coming into contact with tablets or the semen of men taking themReduce PSA by 50%, must interpret PSA in light of this.Most effective when used in combination with alpha 1 blockers.Use results in a 25% reduction in risk of prostate cancer; but a 27% increase in number of highly aggressive tumors among those detected
16. Other TherapiesPhosphodiesterase-5 InhibitorsOctober 2011, the FDA approved tadalafil (Cialis®) for the treatment of symptoms related to BPH. Not first line, but option for men with BPH and EDHypotension risk?AntimuscarinicsAdjunctive for some men with urge incontinenceNot for patients with high post-void residuals
17. Surgical TherapyTypically reserved for men with complications, severe symptoms unresponsive to optimal pharmacotherapy, or those who prefer surgeryGreatly improves symptoms but high complication ratesTransurethral resection of the prostate (TURP)Open prostatectomy
18. The Role of the PharmacistSelecting an agent and appropriate dosePatient education on lifestyle modificationsCounseling on correct administration and management of adverse effectsMonitoring use of OTC and prescription drugs that may exacerbate BPHLink: Table on Monitoring of Drugs Used in Treatment of Benign Prostatic HyperplasiaLink: Table on Dosing of Drugs Used in Treatment of Benign Prostatic Hyperplasia