
Type 2 Idiopathic ductcentric pancreatitis GELs granulocite ephitelial lesions IgG4 Related Diseases Various organ manifestations of a fibroinflammatory condition c haracterized by ID: 774723
Download Presentation The PPT/PDF document " RECAP: Autoimmune Pancreatitis" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.



Slide1
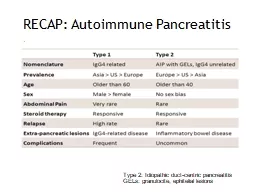
RECAP: Autoimmune Pancreatitis
Type 2: Idiopathic duct-centric pancreatitis
GELs: granulocite, ephitelial lesions
Slide2IgG-4 Related Diseases
Various
organ
manifestations of a fibro-inflammatory
condition
c
haracterized by
tumefactive lesions
recognised as a
systemic condition
in 2003
Linked by the
same histopathological characteristics
and
elevated serum IgG4
concentrations.
Multiple immune-mediated
mechanism contribute to the fibro-inflammatory process, being autoimmunity and infectious agents potential triggers of a Th-2 and T-reg response.
Slide3Pathophysiology
Stone J, Zen Y. IgG4-Related Disease N Engl J Med 2012;366:539-51.
Slide4IgG-4 Related Diseases
Slide5IgG-4 Related Pancreato-biliary Diseases
Majority of patients are men (60-73%), > 60 years
Prevalence 0,2-0,8/100.000
Lack of familiarity!
Up to 40% of patients have
allergic diseases
(atopy, eczema, asthma, chronic sinusitis)
30%
normal
serum IgG-4 concentrations
IgG-4 related
sclerosing cholangitis
associated with AIP in 47–92% of pt
Slide6IgG-4 Pancreatitis
Clinical presentation Acute vs Chronic symptoms Painless obstructive jaundice 33–60% Steatorrhea - exocrine functional abnormalities in up to 80% Abdominal pain 32% Back pain and weight loss 15% Serologic marker: titers of g-globulin (>2000 mg/dL) IgG (>1800 mg/dL) IgG4 (>140 mg/dL)
Serum IgG4 >140 mg/dL
86% SN, 96% SP
Slide7IgG-4 Pancreatitis
Imaging features Enlarged pancreas “sausage-like appareance” 50-70% Focal masses 30% Soft tissue hypoenhancing rim Narrowing of main pancreatic duct “Duct-penetrating” sign at secretin-MRCP
Slide8IgG4 Pancreatitis: DD
Slide9IgG-4 Pancreatitis
Role of EUS-FNA Histological proof of the disease: GOLD STANDARD Exclusion of carcinoma Discrimination of type 1 from type 2 AIP
IgG4-positive plasma cells> 10/hpf
Diffuse lymphoplasmacytic
infiltration and storiform fibrosis
Slide10IgG-4 Pancreatitis
Hystology is the GOLD STANDARD:
Diffuse
lymphoplasmacytic
infiltration with mild-moderate
eosinophilia
Obliterative flebitis
and
storiform fibrosis
IgG4 immunostaining:
> 50 IgG4 plasma cells/HPF for surgical specimens
> 10 IgG4 plasma cells/HPF for biopsy samples
Ratio
IgG4
-positive/
IgG
-positive plasma cells > 40%
Slide11Storiform Fibrosis
Slide12IgG-4 Pancreatitis: diagnosis
The MAYO Clinic HISORt criteria
Slide13IgG-4 Cholangitis
Clinical presentation
70%
obstructive jaundice with pruritus and abdominal pain
Asymptomatic
jaundice less common than AIP
7-10%
cirrhosis
manifestation (hepatic failure, ascites, hepatic encephalopathy or variceal bleeding)
Serologic marker:
titers of g-globulin (>2000 mg/dL)
IgG (>1800 mg/dL)
IgG4 (>140 mg/dL)
reumatoid factor, antinucleus antibody
Slide14IgG-4 Cholangitis
Imaging features Isolated intrapancreatic CBD strictures Localized hilar hepatic lesion (strictures or masses) Intense and diffuse extension of bile duct wall homogeneous thickening (often circular) IDUS: inflamed submucosa and preserved epithelium, circular symmetric wall thickening
Slide15IgG-4 Cholangitis DD
IDUS:
eccentric wall thickening with an irregular luminal surface, disruption of the bile duct wall layered structure, and a hypoechoic mass with irregular margins
Slide16IgG-4 Cholangitis DD
IDUS: all bile duct layers inflamed, bile duct epithelium severely damaged, disappearance of the three layersImaging: diverticulum-like out-pouching, and beaded - tree appearance
Slide17INDUCTION 0,6-1 mg/kg oral prednisolone TAPERING 5 mg/wk reduction MAINTENANCE: 2,5-5 mg/die oral prednisolone or AZA Pancreatic enzyme supplementation (pancrelipasis) for exocrine insufficiency if: steatorrhoea, weight loss, metabolic bone disease, vitamin deficiency Oral hypoglicemic agents or insulin for diabetes mellitus Biliary stenting in obstructive jaundice (case-by-case)
Therapy
Slide18Outcomes
Spontaneous resolution in up to 30%
Response to steroid therapy in 90% to 95% with improvement of imaging findings and serology within 2 weeks + symptoms regression
New onset diabetes mellitus usually improves with corticosteroid therapy
Chronic pancreatitis
in about 10%
Very rarely
progression to cirrhosis in IgG-4 cholangitis
Slide19Outcomes
Response to steroid therapy in 90% to 95% of both parenchymal and ductal changes
Before (A) steroid therapy and after (B)
Slide20Suspect!May have acute or chronic manifestationTypical imaging findings (CT/MRI)Mandatory is exclusion of carcinomaCharacteristic histopathological appearance: histology is the GOLD STANDARDNot always elevated IgG and IgG-4 levelsSystemic disease: look for biliary and retroperitoneal involvement
TAKE HOME MESSAGES
Slide21Stone J, Zen Y. IgG4-Related Disease N Engl J Med 2012; 366: 539-51. Kamisawa T, Zen Y. Advances in IgG4-related pancreatobiliary diseases. Lancet Gastroenterol Hepatol 2018; 3: 575–85. Sandrasegaran K, Menias C. Imaging in Autoimmune Pancreatitis and Immunoglobulin G4–Related Disease of the Abdomen. Gastroenterol Clin N Am. 2018. Article in press.
Bibliografia