
Rajiv Doddamani PGY 3 Internal Medicine St Joseph Mercy Ann Arbor Learning objectives Explain the principles of breast cancer screenings ID: 929035
Download Presentation The PPT/PDF document "BREAST CANCER FOR THE INTERNIST" is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.







Slide1
BREAST CANCER FOR THE INTERNIST
Rajiv Doddamani
PGY – 3, Internal Medicine
St. Joseph Mercy Ann Arbor
Slide2Learning objectives
Explain the principles of breast cancer screenings
Know
when to refer a patient for genetic testing and to a high risk clinic Describe the goals of chemo-prevention Be aware of the modalities of local treatment of breast cancer Know the options of adjuvant systemic therapy and generally when they are used Understand in general the sequence of therapy for metastatic disease Be familiar with the principles of survivorship
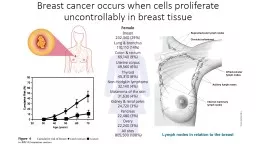
Slide3Overview of breast cancer in the US
Slide4Slide5Screening
Test to detect early stage or pre-cancer lesions in an asymptomatic individual
Test should result in improved disease specific survival
Good example is cervical cancer screening
Slide6Screening – Why do we use mammograms for screening?
Slide7Screening
Prevention group
Age 40-44
Age 45-54 >55American Cancer SocietyIndividualized decisionAnnual Switch to every 2 years or continue annuallyACOG Annual Annual Annual USPSTFIndividualized decision (Grade C)Individualized decision (Grade C)Every 2 years (50-74) (Grade B)ACRAnnual
AnnualAnnual
Slide8Screening tools - Mammogram
Single most effective technique to detect breast cancer before it becomes palpable
Overall sensitivity is about 85%
Principle - Low dose X-rays of breast tissueDiagnostic vs Screening – Primary difference is based on the reason for the exam Diagnostic mammogram may include additional images BI – RADS (Breast Imaging Reporting and Data System)
Slide9Slide10Screening
We do not do ultrasounds alone – Very sensitive, not specific
For women with very dense breasts, ABVS (automated breast volume scanner) may be helpful. If you are not sure, contact one of the breast imaging radiologists to discuss if this could help your patient
Scenario: A 38 year-old woman who felt a mass on self-breast exam. A diagnostic mammogram revealed no evidence of diseaseNext step: USG guided-biopsy
Slide11High risk populations
Known BRCA mutations
Multiple family members with breast and/or ovarian cancer or a male relative with breast cancer
Benign high risk breast lesions - Atypical hyperplasia or LCIS (lobular carcinoma in-situ)Clinical risk factors Multiple breast biopsies Several risk assessment models (Gail, Claus etc)If they have a known BRCA mutation or >20% lifetime risk based on one of those models, she qualifies for annual breast MRI in conjunction with annual mammogram No evidence for breast MRI or ultrasound alone
Slide12MKSAP – Question 113
A 34-year-old woman is evaluated for a 4-week history of tenderness in her left lower breast. Her paternal grandmother died of ovarian cancer at age 54 years. There is no family history of breast cancer. She has a 2-cm palpable left lower outer breast mass on exam. The remainder of the examination is unremarkable.
Results of complete blood count and serum chemistry panel are normal. A mammogram shows increased density and calcifications at the site of the palpable mass. Ultrasound examination reveals a 1.9-cm
hypoechoic mass. Ultrasound-guided needle biopsy specimens show a high-grade invasive ductal carcinoma, estrogen receptor–negative, progesterone receptor–negative, and negative for HER2 amplification.Which of the following is the most appropriate initial management?A Bilateral mastectomy B BRCA1/2 testingC Left mastectomyD Lumpectomy with sentinel lymph node biopsy
Slide13Who should be tested for BRCA mutations?
Highlights from NCCN guidelines
Family history of known deleterious BRCA 1/2 mutation
Personal history of breast cancer at any age with multiple family members with breast and/or ovarian cancer Ashkenazi Jewish descent Young age at diagnosis (<45 years)Triple negative cancer diagnosed before age <60Personal history of epithelial ovarian cancer Men with breast cancer diagnosed at any age
Slide14Management of high risk patients
BRCA 1 or 2 mutations – Aggressive screening program with annual breast MRI and annual mammogram starting at age 25 OR prophylactic bilateral mastectomy which reduces risk by 90%
Chemoprevention – Use of SERM or aromatase inhibitor to reduce risk of getting breast cancer in patients that are at high risk due to history of AH, LCIS or based on risk model
5 years of therapy Prevents HR+ breast cancer ( risk by about 50%) and not HR- cancer No known survival benefit; just reduces the incidence Tamoxifen, raloxifen or aromatase inhibitors can be used
Slide15Flowchart of a patient’s care
Most women present first to radiology for a screening mammogram or to their PCP with a breast finding (lump, discharge, skin change like nipple retraction etc.)
If you have a patient with a breast finding, you must get a
diagnostic mammogram, ultrasound and biopsy (if palpable lesion)From radiology, the patient will usually a surgeon if the biopsy is proven cancer Surgeon will discuss surgical optionsIf the surgeon wants to have the patient considered for pre-operative systemic treatment, the patient will be sent to medical oncology Radiation oncology usually joins the party after surgery. Not all patients get radiation
Slide16Principles of management
Multidisciplinary approach
Surgery is cornerstone
Chemo and RT – To lower risk of relapse
Slide17Staging
Slide18Principles of surgery
For stages I-III (curative intent)
Crucial role in local control of disease and accurate staging
Breast conservation therapy (BCT) – Lumpectomy (tumor and surrounding tissue removed) plus whole breast radiation therapy Mastectomy – All breast tissue removed Sentinel lymph node biopsy is standard unless there is clinically or radiologically (USG) detectable nodal metastasis Survival is the same with BCT and mastectomy No survival benefit to prophylactic contralateral mastectomy
Slide19Principles of radiation therapy
Why? When? Where?
Helps to achieve goal of local control of the disease (reduces
locoregional recurrence by 50%)Axillary radiation Regional node irradiation Post mastectomy radiation therapy Small benefit in survival Elderly women may be spared
Slide20Role of systemic therapy
For loco-regional disease, systemic therapy is given in addition (adjuvant or neo-adjuvant) to surgery with a curative intent
For metastatic disease, systemic therapy is mainstay of therapy with a palliative intent
Prolong life expectancy Improve symptoms Prevent symptoms from cancer (in asymptomatic individuals) Immunotherapy – In trials for breast cancer Targeted therapy – Anti HER2 therapy, CDK 4/6 inhibitors, P13K inhibitors Endocrine therapy – Tamoxifen, aromatase inhibitors and fulvestrantChemotherapy (Neo-adjuvant, adjuvant and palliative)
Slide21Indications for HER2 therapy
HER – Human epidermal receptor
HER2 overexpression (IHC) or amplification (genetic) is a
predictive marker for response to therapy Prognostic when used in conjunction with ER and PR status Can be used in neoadjuvant, adjuvant or palliative settings Trastuzumab (Herceptin) and pertuzumab (Perjeta) and monoclonal antibodies (IV)Lapatinib is a small molecule inhibitor (oral)
Slide22MKSAP - 148
A 43-year-old woman undergoes follow-up evaluation following a recent diagnosis of estrogen receptor–positive, progesterone receptor–positive, HER2-negative, grade 2 invasive ductal carcinoma of the left breast. The patient was treated with surgery, adjuvant chemotherapy, and radiation therapy. This is her first
postradiation
visit. She currently takes no medications. She is premenopausal.On physical examination, vital signs are normal. Well-healed incisions of the left breast and left axilla are present. There is no lymphadenopathy and no right breast masses. The remainder of the examination is unremarkable.Results of a complete blood count and serum chemistry panel are normal.Which of the following is the most appropriate therapy? A Exemestane aloneB Tamoxifen aloneC Maintenance chemotherapy with oral capecitabineD No additional adjuvant therapy
Slide23Endocrine therapy
Tamoxifen
– SERM which blocks ER receptor in breast tissue
Aromatase inhibitors (AIs) – Inhibit aromatase which is needed to convert androgen to estrogen; thus depletes the body of systemic estrogenFulvestrant – SERD (selective estrogen receptor down-regulator)Tamoxifen – Can be used in pre or post-menopausal women, adjuvant setting (5 years) and palliative (continue as long as it works)Should not take certain SSRIs (fluoxetine) – Interfere with tamoxifen metabolism and reduce its effectivenessAI – Only for use in post-menopausal women Fulvestrant – Approved for post menopausal women
Slide24Cytotoxic chemotherapy
Adjuvant and
neoadjuvant
- CombinationTaxanesDoxorubicin Cyclophosphamide Palliative Single agent sequential chemo
Slide25Genomic assays
Oncotype
DxTM and MammaprintTMUses a panel of genes associated with breast cancer tumor behavior to test a patient’s tumor and come up with a risk of recurrence and a benefit to chemotherapy Spares some patients from getting adjuvant chemotherapy
Slide26Common toxicities
Doxorubicin – Cardiomyopathy
Tamoxifen
– Hot flashes, DVT and endometrial carcinoma (post-menopausal women)AIs – Joint aches, loss of bone density, fatigue, vaginal drynessTrastuzumab – Generally well tolerated, cardiomyopathy in a small number of patients (reversible on cessation of therapy)Pertuzumab - Diarrhea
Slide27Survivorship
An
increasing proportion of cancer patients survive their cancer
Have specific risks related to previous treatments and risks related to other types of cancer as well as unique financial and psychosocial issues Survivorship care plan is now mandated by the Commission on Cancer
Slide28MKSAP 126
A 44-year-old woman undergoes follow-up evaluation. Stage I cancer of the left breast was diagnosed 3 years ago (1.4-cm, grade 2 invasive ductal carcinoma, estrogen receptor positive, progesterone receptor positive, HER2 negative, 0/2 positive sentinel lymph nodes, and a low score on 21-gene recurrence score testing). BRCA1/2 testing results were negative. She underwent breast-conserving surgery and radiation therapy and then started
tamoxifen
. The patient is concerned about her risk of recurrence. Menses are irregular. She has occasional hot flushes and night sweats on tamoxifen but otherwise feels well. There is no family history of breast or ovarian cancer.On physical examination, vital signs are normal. BMI has remained stable at 22.4. Well-healed left breast and left axilla incisions are present. There are no breast masses or lymphadenopathy. The remainder of the examination is unremarkable.Results of a bilateral mammogram obtained 1 month ago were normal.Which of the following is the most appropriate next step in the management of this patient? A Bilateral breast MRIB Complete blood count, liver chemistry studies, and CEA and CA 15-3 measurementC CT of the chest, abdomen, and pelvis and bone scanD No diagnostic studies at this time
Slide29Survivorship
Body image issues – Hair, breasts, skin
Mental health – Depression, anxiety related to risk of recurrence, sleep disturbance
Sexual health/function – Loss of interest, loss of libido Long term SEs from chemotherapy – Neuropathy, cardiomyopathy Long term SEs from XRT and surgery - Chronic pain, risk of second tumorsEndocrine therapy – Joint pain, weight gain Preventative care – Immunizations, physical activity, prevention of 2nd primary cancers, bone density
Slide30Survivorship
Breast exam every 6-12 months and annual breast cancer screening (until life expectancy less than 5 years)
Breast exam – inspection, palpation, nipple examination and regional node exam
Doxorubicin toxicity – Echo q5yrs after chemo PT/OT for neuropathy Utilize psychiatry/psychology for mental health issues Encourage breast cancer support groups for struggling patientsSmoking cessation, limit alcohol intake
Slide31References
NCCN
UpToDate
MKSAP ASCO ESMO