
lthough celiac disease was formally described late in the19th centurytreatment remained empiric until the mid Glutensensitive enteropathy or as it is more commonly called celiac disease is an ID: 953271
Download Pdf The PPT/PDF document "152002 VOLUME66NwwwaafporgafpAMILYHYS..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

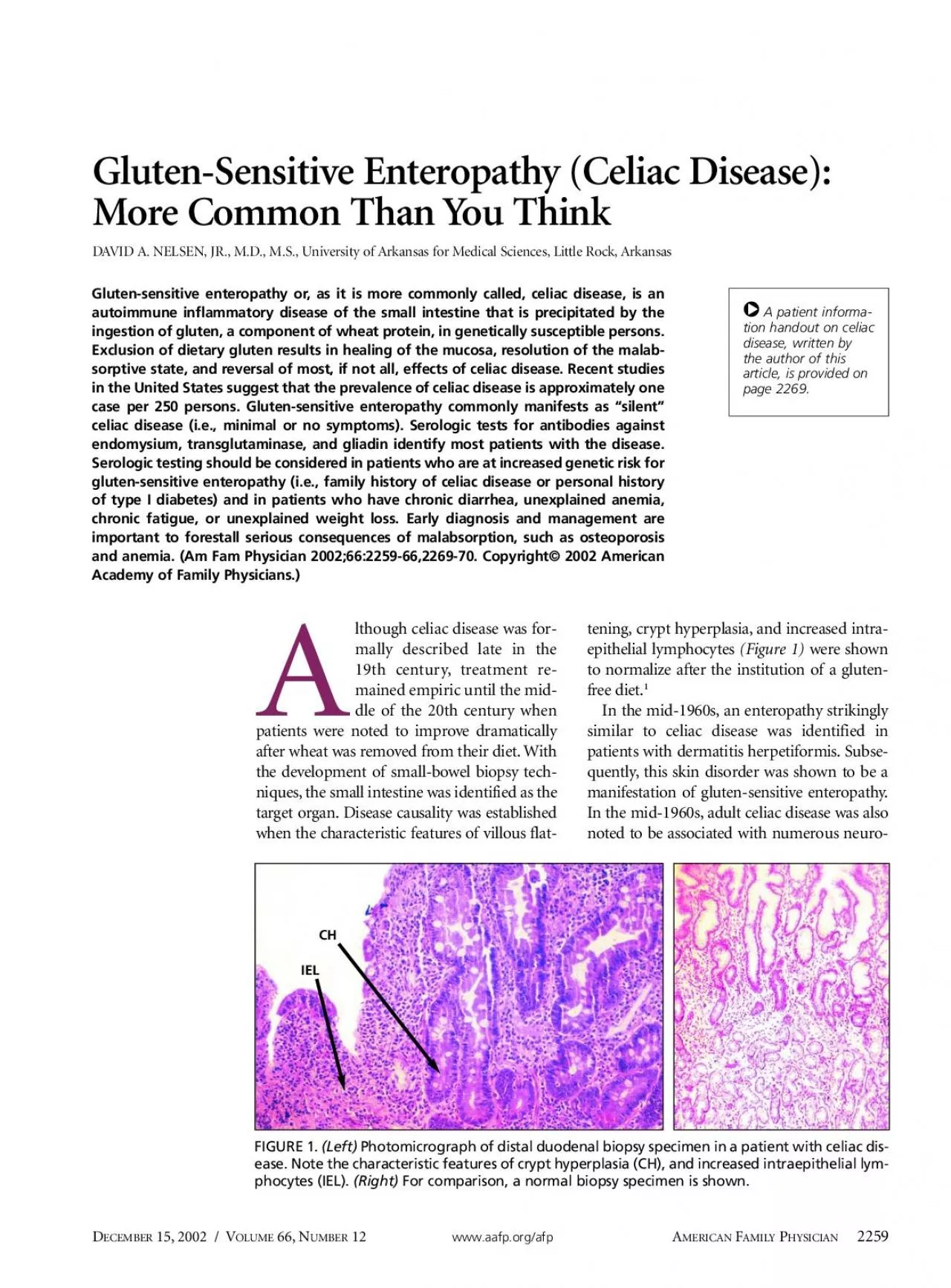
15,2002 / VOLUME66,Nwww.aafp.org/afpAMILYHYSICIAN lthough celiac disease was for-mally described late in the19th century,treatment re-mained empiric until the mid- Gluten-sensitive enteropathy or, as it is more commonly called, celiac disease, is an Gluten-Sensitive Enteropathy (Celiac Disease):mmon Than You Think Photomicrograph of distal duodenal biopsy specimen in a patient with celiac dis- A patient informa-the author of thisarticle, is provided on logic disorders,including epilepsy,cerebral calcifications,and peripheral neuropathy.nt population studies indicate that celiac disease ismore common than was previously thought.Somepatients with gluten-sensitive enteropathy have minimalor no symptoms and are unlikely to be referred to a gas-oenterologist unless the disease is considered.Hence,family physicians need to be familiar with the diagnosisand management ofgluten-sensitive enteropathy.gested protein does not normally provoke animmune response.This phenomenon is termed Òoral tol-erance.ÓPatients who exhibit true allergy to an ingestedprotein (e.g.,milk or soy protein) have a typical IgE-medi-ated response consisting ofurticaria,angioedema,andbronchoreactivity.The autoimmunity in gluten-sensitive enteropathyinvolves plasma cells that produce IgA and IgG;there is lit-tle or no IgE involvement.Current theory suggests thatingested -gliadin (a component ofthe gluten protein)and related peptides bind with tissue transglutaminase (a ubiquitous intracellular enzyme) in enterocytes.The -gliadin is rich in glutamine;transglutaminase deami-dates glutamine residues,forming glutamic acid.Deami-dation enhances the immunogenicity of-gliadin by cre-ating epitopes that are recognized as foreign by hostllÐmediated immunity.Plasma cells produce IgA and IgG that are directedagainst a variety ofantigens,including transglutaminase,endomysium,gliadin,and reticulin.Locally elaboratedlymphokines attract inflammatory cells.This intenselocal inflammatory reaction produces the villous flatten-ing characteristic ofgluten-sensitive enteropathy.Malab-sorption ofmicronutrients (e.g.,vitamins and minerals)and macronutrients (e.g.,protein,carbohydrate,fat) fol-lows.Small-bowel involvement is most prominent proxi-mally and may be Òpatchy,Óespecially in patients withsilentÓceliac disease (i.e.,minimal or no symptoms) andthose with dermatitis herpetiformis.pproximately 95 percent ofpatients with celiac diseaseexhibit specific Human Leukoce Antigen (HLA) class IIalleles DQA1*0501 and DQB1*0201.tients with type 1diabetes,autoimmune thyroid disease,SjgrenÕs syn-drome,primary biliary cirrhosis,AddisonÕs disease,sys-mic lupus erythematosus,selective IgA deficiency,andalopecia areata may also exhibit similar genotypes and areat risk for gluten-sensitive enteropathy (Table 1).many persons have these genotypes and only a few developuten-sensitive enteropathy,investigators have hypothe-sized that other genes or cofactors may be involved.til recently,celiac disease was considered to be rela-tively uncommon.Previous U.
S.figures suggested that itaffected one in 6,000 persons.published in the past four years suggest a much higherprevalence,particularly in persons ofEuropean ancestry.Studies conducted in Europe estimate the seroprevalence ofliac disease to be one case per 130 to 300 persons.In a rent U.S.study,investigators tested sera from2,000 healthy Red Cross blood donors and found eightsamples that were positive for antibodies associated withuten-sensitive enteropathy (seven samples from whiteAMILYHYSICIANwww.aafp.org/afpOLUME66,N12 / D15,2002 ABLE 1 Celiac Disease and Other Autoimmune Disorders*Autoimmune thyroid diseaseSystemic lupus erythematosus Autoimmune AddisonÕs disease*ÑListed in descending order of clinical importance and prevalence. Observed association.Recurrent aphthous ulcerationsSjgrenÕs syndromeSarcoidosisitiligo or alopecia areata DAVID A. NELSEN, JR., M.D., M.S., is associate professor in the Depart-Medical Sciences, Little Rock, where he earned his medical degree andcompleted a family medicine residency. He completed a faculty develop-Medical School, Minneapolis, where he also earned a masterÕs degree infamily and community medicine. Dr. Nelsen has published and presentedin the area of medical informatics and speech recognition. He serves onAddress correspondence to David A. Nelsen Jr., M.D., M.S., Universitynity Medicine, Mail Slot #530, 4301 W. Markham, Little Rock, ARfrom the author. persons,one sample from a black person).The seropreva-lence rate in this study (one case per 250 persons tested) isnsistent with the rates in European studies.The likelihood ofhaving gluten-sensitive enteropathyincreases to 10 to 20 percent in persons who have a first-degree relative with celiac disease.addition,celiac dis-ease is associated with other autoimmune syndromes.Forxample,as many as 7 percent ofpatients with type I dia-betes also have gluten-sensitive enteropathy.Clinical Presentationeated gluten-sensitive enteropathy is associated witha range ofsymptoms(Table 2).The ÒclassicÓform typi-cally presents in infancy and manifests as failure to thrive,diarrhea,abdominal distention,developmental delay,and,occasionally,severe malnutrition.Failure to diagnose thedisorder may lead to a true medical emergency.Beyond infancy,the symptoms ofceliac disease tend tobe less dramatic.Older children may present with consti-tutional short stature or dental enamel defects.men comprise approximately 75 percent ofnewlydiagnosed adult celiac disease cases.Women also tend tohave more clinically conspicuous disease.both sexes,gastrointestinal tract involvement may mani-fest as diarrhea,constipation,or other symptoms ofmal-absorption,such as bloating,flatus,or belching.Fatigue,depression,fibromyalgia-like symptoms,aphthous stoma-titis,bone pain,dyspepsia,gastroesophageal reflux,andother nonspecific symptoms may be present and canmake the diagnosis quite challenging.A number ofotherautoimmune syndromes have been associated with celiac(Table 1).DERMATITISHERPETIFORMISr than 10 percent ofadults with gluten-
sensitiveenteropathy present with dermatitis herpetiformis.skin condition may be misdiagnosed as atypical psoriasisor nonspecific dermatitis.The rash ofdermatitis herpetiformis is intensely pruriticand typically occurs on the back,buttocks,knees,andelbows (Figure 2).iated lesions (Figure 3)are15,2002 / VOLUME66,Nwww.aafp.org/afpAMILYHYSICIAN ABLE 2 SymptomsPossible causesFatigue, malaiseAnemia, general immune system ight lossNutrient malabsorptionDiarrhea, abdominal Accelerated gastrointestinal tract paintransit time, steatorrhea, AnemiaMost commonly, iron deficiency; less commonly, vitamin Band/or folate Bone painOsteoporosisAphthous oral ulcers, Vitamin deficiency, ÒoralÓ celiac diseaseglossitis, stomatitisInfertilityPostulated cause: iron, folate, and/or Male impotence, Peripheral insensitivity to circulating decreased libidotestosteroneAlopecia areataImmunologic attack on hair folliclesDental enamel defectsDemineralization during tooth bud development in childrenHypoglycemiaDelayed absorption of glucoseintestinal floraSeizures, gluten ataxia, Increased affinity of celiac antibodies central nervous systemfor brain vasculature symptoms Fewer than 10 percent of adults with gluten-sensitive enteropathy present with dermatitis herpetiformis. Òceliac disease of the skin.Ó Vesicular, crusted, intensely pru- markably like those ofherpes simplex (thus,the termerpetiformisÓ).Granular IgA deposition on immunoflu-orescence ofa skin biopsy specimen is diagnostic (Figure 4).emia is the most common laboratory manifestation of(Table 3).One halfofpatients with newlydiagnosed gluten-sensitive enteropathy are anemic.Iron isabsorbed in the proximal small intestine,where celiac man-ifestations are most prominent;hence,iron malabsorption ismmon.In addition,occult blood loss related to intensesmall-bowel inflammation may occur in 50 percent ofpatients with gluten-sensitive enteropathy.ess com-monly,vitamin Bdeficiency,folate deficiency,or both maybe present.SILENTCELIACDISEASEA number ofinvestigators believe that clinically apparent gluten-sensitive enteropathy represents the Òtip ofthe icebergÓofthe overall disease burden.who were detected in the seroprevalence studieswereasymptomatic or oligosymptomatic (so-called ÒsilentÓamily physicians should consider serologic testing inpatients with the following:family history ofceliac dis-ease,personal history ofthyroid disease or type I diabetes,irritable bowel syndrome,anemia (especially iron defi-ciency),chronic diarrhea,chronic fatigue,unexplainedight loss,short stature,epilepsy,infertility,or unex-plained elevation oftransaminase levels.Asymptomatic oroligosymptomatic patients are still at risk for complica-tions ofceliac disease.SEROLOGICTESTSen the diagnosis ofgluten-sensitive enteropathy is sus-pected,serologic tests can identify many affected patients.(Figure 5).gA antiendomysial antibody has been shown tobe 85 to 100 percent sensitive and 96 to 100 percent specificfor celiac disease.IgA antiendomysial antibody is measuredusing direct immunofluor
escence ofmonkey esophagus orumbilical cord tissue processed with suspect serum.gG and IgA antigliadin antibodies are also useful indiagnosing celiac disease.The antibody directed againstendomysium has recently been identified as identical to theantibody directed against (tissue) transglutaminase.Anenzyme-linked immunosorbent assay has been developedmeasure IgA antitransglutaminase;this test will gener-ally replace the more tedious direct fluorescent antibodyest for IgA antiendomysial antibody.diagnosingliac disease,antitransglutaminase antibody is consideredbe approximately as sensitive and specific as antien-domysial antibody (Table 4).The presence ofIgA antiendomysial and antitransglutam-inase antibodies correlates with intestinal damage.Tests forthese antibodies are highly sensitive in patients with totalAMILYHYSICIANwww.aafp.org/afpOLUME66,N12 / D15,2002 FIGURE 3. Close-up view of dermatitis herpetiformis. Unex-coriated lesions are remarkably like those of herpes sim-plex (thus, the term ÒherpetiformisÓ). FIGURE 4. Photomicrograph of a skin biopsy specimen in apatient with dermatitis herpetiformis. Note the intenseinflammatory infiltration at the dermoepidermal junction.Immunofluorescence demonstrated granular deposition ofIgA (arrow). IgA antiendomysial antibody has been shown to be 85 to 100 percent sensitive and 96 to 100 and subtotal villous atrophy.IgA antiendomysial antibodyesting has been reported to be 100 percent sensitive inpatients with total villous atrophy.The combination ofIgAantiendomysial antibody and IgG and IgA antigliadin anti-bodies detects 76 percent ofpatients with mucosal damage.is important to note that 2 to 3 percent ofpatientsith gluten-sensitive enteropathy also have selective IgAdeficiency.Because these patients may not produce thediagnostic IgA antibodies,a positive IgG antigliadin anti-body test may be the only serologic evidence ofthe dis-ease.Ifclinical suspicion is high,quantitative IgA mea-surements should be obtained in these patients.Endoscopy and biopsy should be strongly considered inpatients with selective IgA deficiency.15,2002 / VOLUME66,Nwww.aafp.org/afpAMILYHYSICIAN ABLE 3 Laboratory findingPathophysiologyAnemiaIron deficiency; vitamin BElevated alkaline phosphatase Osteoporosis, osteomalaciaElevated aspartate transaminase Minimal elevation common transaminasein celiac disease; presumably levelsautoimmune Decreased albumin levelMalnutritionElevated calcium level, decreased Vitamin D deficiency, secondary phosphate levelhyperparathyroidismThrombocytosis, leukocytosisGeneral inflammatory reactionCoagulopathyDecrLow high-density and low-density Decrlipoprotein cholesterol levels decreased hepatic lipoprotein production Clinical suspicion: patient with symptoms or risk factors suggestive of gluten-sensitive enteropathy (celiac disease)Quantitative IgA measurementsIntermediate probabilityPlan EGD, with or withoutHigh probability Low probability is high, consideror EGD.High probability of celiac diseaseIgA normalIgA deficientSerologic
testing:IgA antigliadin antibodyIgG antigliadin antibodyIgA antiendomysial antibody FIGURE 5. Algorithm for the diagnosis of celiac disease. (EGD = esophagogastroduodenoscopy) Declining autoantibody titers correlate with resolution ofthe gastrointestinal lesion and may be used to document clin-ical improvement.In equivocal cases or when a patient hasbeen on a gluten-free diet,a gluten challenge test may be usedprovoke the gastrointestinal lesion and serologic response.DISTALDUODENALBIOPSYDistal duodenal biopsy is the gold standard for the diag-nosis ofceliac disease.Biopsy should be performed inmost patients with suspected gluten-sensitive enteropathy.determining the need for biopsy,family physiciansshould consult a gastroenterologist who is experienced inthe diagnosis and management ofceliac disease.Calcium and vitamin D malabsorption dramaticallyincreases the risk ofosteoporosis and osteomalacia inpatients with gluten-sensitive enteropathy.Most patientsith celiac disease have some degree ofosteopenia orosteoporosis.Fortunately,calcium and vitamin D supple-mentation,coupled with a strict gluten-free diet,usuallysults in remineralization ofthe skeleton.Bone density should be assessed in all patients withnewly diagnosed celiac disease.Postmenopausal womenshould be advised about the benefits ofestrogen replace-ment.The use ofantiresorptive agents (e.g.,alendronate[Fosamax]) has not been extensively studied,but thesedrugs may be ofbenefit.NEUROLOGICMANIFESTATIONSCerebral calcifications and epilepsy have been associ-ated with celiac diseaseand do not always resolve withthe institution ofa gluten-free diet.Peripheral neuropa-thy,postural instability,Ògluten ataxia,Óand other vagueneurologic complaints may be the sole manifestation ofuten-sensitive enteropathy.antibodies associatedith celiac disease have demonstrated a strong affinity forbrain vasculature.REFRACTORYSPRUEpatients with refractory sprue,gastrointestinal tractinflammation continues despite maintenance ofa gluten-free diet.Dietary noncompliance is the most commoneason for persistent inflammation;however,coexistentnditions such as hyperthyroidism and collagenous coli-tis should also be considered.tients who are truly refractory to dietary measuresmay have cryptic lymphoma of(bowel) intraepitheliallymphocytes.All diet-refractory patients should be evalu-ated by a gastroenterologist with expertise in the manage-ment ofceliac disease.Corticosteroids and immunosup-pressant drugs have been used to treat refractory sprue,but data on their effectiveness are sparse.estinal strictures and bowel obstruction may developin patients with refractory sprue or celiac disease that hasbeen untreated over a long period.YMPHOMAANDBOWELADENOCARCINOMAEnteropathy-associated T-cell lymphoma has been asso-ciated with untreated gluten-sensitive enteropathy andrefractorysprue.Lymphoma may develop in patientsith celiac disease who also have dermatitis herpetiformis.have shown that maintenance ofa long-uten-free state reduces the risk oflymphoma to the
level in the general population.Thus,it is imperative thatAMILYHYSICIANwww.aafp.org/afpOLUME66,N12 / D15,2002 ABLE 4 Serologic Tests for Celiac Disease Antibody testSensitivity (%)Specificity (%)Time courseCostIgA antiendomysial 85 to 10096 to 100Antibody disappears within several months after $45 to 99antibodyinstitution of gluten-free diet.IgA antitransglutaminase 9590Limited data; correlated with IgA antiendomysial 85 to 164antibodyantibody in studiesIgA antigliadin antibody53 to 10065 to 100More persistent than IgA antiendomysial antibody; 45may persist for 6 months or longerIgG antigliadin antibody57 to 10042 to 98Most persistent; may be detectable up to 12 months 45 to 90after institution of gluten-free dietFalse-positive tests reported in patients with CrohnÕs disease, wheat-protein allergy, and verage of costs at three reference laboratories in the summer of 2001. Information from references 21 through 23 and 25 patients with celiac disease (and dermatitis herpetiformis)maintain a gluten-free diet for the rest oftheir lives.tients with celiac disease are also at risk for the devel-opment ofbowel adenocarcinoma in all sites.The risk isespecially high in patients with a long period ofdiseasepreceding institution ofa gluten-free diet.Once the diagnosis ofceliac disease has been made,patients should be evaluated for known manifestations andcompli(Table 5)n deficiency should be treatedith supplemental iron.Osteoporosis should be treatedith calcium and vitamin D replacement.Depending onindividual factors,patients with gluten-sensitive enteropa-thy may need to take a multivitamin,iron,calcium,magne-sium,zinc,selenium,vitamin D,or other nutrients.The primary treatment for celiac disease is the removalofgluten and related proteins from the diet.Completeclusion ofdietary gluten generally results in rapid andmplete healing ofsmall-bowel inflammation.Advicefrom a registered dietitian is essential to outline an appro-priate diet.Gluten,a prolamine,is the primary protein in wheat.nce,wheat and products containing wheat must beoided.Barley and rye contain similar proteins and mustalso be avoided.Oats are a subject ofcontroversy.Although oats themselves may be nontoxic in limitedquantities,commercial oat products are measurably con-taminated with wheat.Rice,corn,maize,flax,quinoa,tapioca,potato,amaranth,and other grain substitutes,such as nuts and beans,are safe.There are many commercial gluten-free products,including breads,cookies,chips,and cereals,that can beused to fashion a rich and interesting diet.Meats,vegeta-bles,fruit,and most dairy products are free ofgluten,as long as they have not been contaminated during production.A number offood manufacturers maintain lists ofuten-free products.These lists can be obtained from themanufacturersÕWeb sites or by telephone request.Infor-mation on gluten-free foods is also available from local ornational support groups such as the Celiac Sprue Associa-tion.Selected resources are provided in Table 6.est. Sources of funding: none reported. Fig
ure 1 provided by Laura Lamps, M.D., assistant professor ofpathology, University of Arkansas for Medical Sciences (UAMS),Little Rock. Figure 4 provided by Bruce Smoller, M.D., professor ofpathology and dermatology, UAMS.15,2002 / VOLUME66,Nwww.aafp.org/afpAMILYHYSICIAN ABLE 5 Iron level, total iron-binding capacity determination, ferritin level*Calcium and phosphate levelsBlood urea nitrogen and creatinine levelsAlbumin and total serum protein levelsDual energy x-ray absorptiometry (DEXA) of spine and hipSerologic testsQuantitative IgA antiendomysial antibody or quantitative IgA Quantitative IgA and IgG antigliadin antibodies*ÑThe ferritin level may be misleading: it may be elevated as an tives of patients with newly diagnosed celiac disease. TABLE 6 Selected ResourcesCeliac Sprue Association/United States of America, Inc.*O. Box 31700, Omaha, NE 68131-0700lephone: 402-558-0600Fax: 402-558-1347eb site: www.csaceliacs.org E-mail address: celiacs@csaceliacs.orgCeliac Discussion List Archiveseb site: www.fastlane.net/homepages/thodge/ archive.shtmlNational Digestive Diseases Information Clearinghouseeb site: www.niddk.nih.gov/health/digest/pubs/celiac/index.htmCeliac Disease Resources for Medical Professionals eb site: www.uams.edu/celiacDavid A. Nelsen, Jr., M.D., M.S., maintains a Web site withresources for primary care physicians to assist them in the care of patients with celiac disease. Celiac Disease 1.Ciclitira PJ, King AL, Fraser JS. AGA technical review on celiacsprue. American Gastroenterological Association. Gastroenterol-2.Van De Wal Y, Kooy Y, Van Veelen P, Vader W, Koning F, Pena S.Coeliac disease: it takes three to tango! Gut 2000;46:734-7.3.Marsh MN. The natural history of gluten sensitivity: defining, refin-ing and re-defining. QJM 1995;88:9-13.4.Sollid LM, Markussen G, Ek J, Gjerde H, Vartdal F, Thorsby E. Evi-HLA-DQ alpha/beta heterodimer. J Exp Med 1989;169:345-505.Collin P, Salmi J, Hallstrom O, Reunala T, Pasternack A. Autoim-mune thyroid disorders and coeliac disease. Eur J Endocrinol 1994;6.American Gastroenterological Association medical position state-ment: celiac sprue. Gastroenterology 2001;120:1522-25.7.Catassi C, Ratsch IM, Fabiani E, Rossini M, Bordicchia F, Candela F,8.Fasano A, Catassi C. Current approaches to diagnosis and treat-ment of celiac disease: an evolving spectrum. Gastroenterology9.Hin H, Bird G, Fisher P, Mahy N, Jewell D. Coeliac disease in pri-mary care: case finding study. BMJ 1999;318:164-7.10.Branski D, Troncone R. Celiac disease: a reappraisal. J Pediatr11.Not T, Horvath K, Hill ID, Partanen J, Hammed A, Magazzu G, etal. Celiac disease risk in the USA: high prevalence of antiendomy-sium antibodies in healthy blood donors. Scand J Gastroenterol12.Cronin CC, Shanahan F. Insulin-dependent diabetes mellitus and13.Iovino P, Ciacci C, Sabbatini F, Acioli DM, DÕArgenio G, MazzaccaAm J Gastroenterol 1998;93:1243-9.14.Clemens, PC. Coeliac disease in adults with atypical symptomsClemens, PC. Coeliac disease in adults with atypical symptoms1
5.Ciacci C, Cirillo M, Sollazzo R, Savino G, Sabbatini F, Mazzacca G.Gender and clinical presentation in adult celiac disease. Scand JGastroenterol 1995;30:1077-81.16.Trier JS. Celiac sprue and refractory sprue. In: Feldman M, FordtranJS, Sleisenger MH, Scharschmidt BF, eds. Sleisenger & FordtranÕsGastrointestinal and liver disease: pathophysiology, diagnosis,17.Fine KD. The prevalence of occult gastrointestinal bleeding in18.Sher KS, Mayberry JF. Female fertility, obstetric and gynaecologicalhistory in coeliac disease. A case control study. Digestion 1994;19.Fotoulaki M, Nousia-Arvanitakis S, Augoustidou-Savvopoulou P,Kanakoudi-Tsakalides F, Zaramboukas T, Vlachonikolis J. Clinical20.Troncone R, Maurano F, Rossi M, Micillo M, Greco L, Auricchio R,et al. IgA antibodies to tissue transglutaminase: an effective diag-21.Vitoria JC, Arrieta A, Arranz C, Ayesta A, Sojo A, Maruri N, et al.for the diagnosis of celiac disease. J Pediatr Gastroenterol Nutr22.Dieterich W, Ehnis T, Bauer M, Donner P, Volta U, Riecken EO, et23.Biagi F, Ellis HJ, Yiannakou JY, Brusco G, Swift GL, Smith PM, et al.troenterol 1999;94:2187-92.24.Russo PA, Chartrand LJ, Seidman E. Comparative analysis of sero-logic screening tests for the initial diagnosis of celiac disease. Pedi-25.Valdimarsson T, Franzen L, Grodzinsky E, Skogh T, Strom M. Isease and IgA anti-endomysium antibodies? 100% positive predic-26.Cataldo F, Marino V, Bottaro G, Greco P, Ventura A. Celiac diseaseand selective immunoglobulin A deficiency. J Pediatr 1997;131:27.Valdimarsson T, Lofman O, Toss G, Strom M. Reversal of osteope-28.Sategna-Guidetti C, Grosso SB, Grosso S, Mengozzi G, Aimo G,Zaccaria T, et al. The effects of 1-year gluten withdrawal on bone29.Dickey W. Epilepsy, cerebral calcifications, and coeliac disease.30.Hadjivassiliou M, Chattopadhyay AK, Davies-Jones GA, Gibson A,Grunewald RA, Lobo AJ. Neuromuscular disorder as a presentingfeature of coeliac disease. J Neurol Neurosurg Psychiatry 1997;63:31.Hadjivassiliou M, Grunewald RA, Chattopadhyay AK, Davies-JonesGA, Gibson A, Jarratt JA, et al. Clinical, radiological, neurophysio-logical, and neuropathological characteristics of gluten ataxia.32.Pratesi R, Gandolfi L, Friedman H, Farage L, de Castro CA, CatassiC. Serum IgA antibodies from patients with coeliac disease reactstrongly with human brain blood-vessel structures. Scand J Gas-troenterol 1998;33:817-21.33.Pricolo VE, Mangi AA, Aswad B, Bland KI. Gastrointestinal malig-34.Lewis HM, Renaula TL, Garioch JJ, Leonard JN, Fry JS, Collin P, etal. Protective effect of gluten-free diet against development oflymphoma in dermatitis herpetiformis. Br J Dermatol 1996;35.Holmes GK, Prior P, Lane MR, Pope D, Allan RN. Malignancy incoeliac diseaseÑeffect of a gluten free diet. Gut 1989;30:333-8.36.Hoffenberg EJ, Haas J, Drescher A, Barnhurst R, Osberg I, Bao F, etal. A trial of oats in children with newly diagnosed celiac disease.37.Janatuinen EK, Pikkarainen PH, Kemppainen TA, Kosma VM, Jarvi-AMILYHYSICIANwww.aafp.org/afpOLUME66,N12 / D15,2