
Scope All critically ill paediatric patients Adapted from Scotstar Website M MacKinnon 22112016 Raigmore Critical Care Guidelines Paediatric Asthma Guidelines Child with Asthma referred to Critical Care ID: 1038217
Download Presentation The PPT/PDF document "Aim To provide guidance on initia..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.


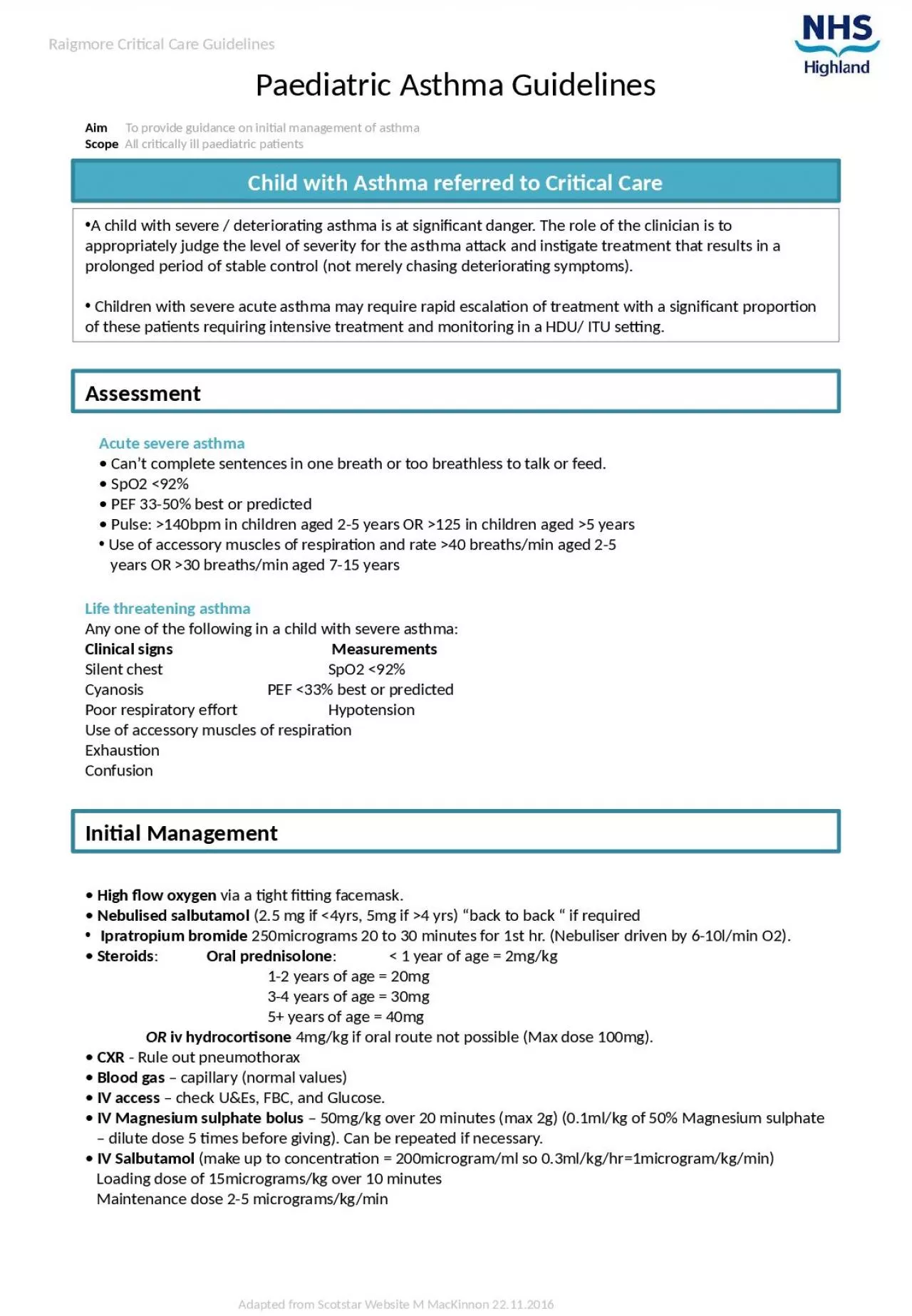
1. Aim To provide guidance on initial management of asthmaScope All critically ill paediatric patientsAdapted from Scotstar Website M MacKinnon 22.11.2016Raigmore Critical Care GuidelinesPaediatric Asthma GuidelinesChild with Asthma referred to Critical CareA child with severe / deteriorating asthma is at significant danger. The role of the clinician is to appropriately judge the level of severity for the asthma attack and instigate treatment that results in a prolonged period of stable control (not merely chasing deteriorating symptoms). Children with severe acute asthma may require rapid escalation of treatment with a significant proportion of these patients requiring intensive treatment and monitoring in a HDU/ ITU setting.AssessmentAcute severe asthma• Can’t complete sentences in one breath or too breathless to talk or feed.• SpO2 <92%• PEF 33-50% best or predicted• Pulse: >140bpm in children aged 2-5 years OR >125 in children aged >5 years Use of accessory muscles of respiration and rate >40 breaths/min aged 2-5years OR >30 breaths/min aged 7-15 yearsLife threatening asthmaAny one of the following in a child with severe asthma:Clinical signs MeasurementsSilent chest SpO2 <92%Cyanosis PEF <33% best or predictedPoor respiratory effort HypotensionUse of accessory muscles of respirationExhaustionConfusionInitial Management• High flow oxygen via a tight fitting facemask.• Nebulised salbutamol (2.5 mg if <4yrs, 5mg if >4 yrs) “back to back “ if required Ipratropium bromide 250micrograms 20 to 30 minutes for 1st hr. (Nebuliser driven by 6-10l/min O2).• Steroids: Oral prednisolone: < 1 year of age = 2mg/kg 1-2 years of age = 20mg 3-4 years of age = 30mg 5+ years of age = 40mg OR iv hydrocortisone 4mg/kg if oral route not possible (Max dose 100mg).• CXR - Rule out pneumothorax• Blood gas – capillary (normal values)• IV access – check U&Es, FBC, and Glucose.• IV Magnesium sulphate bolus – 50mg/kg over 20 minutes (max 2g) (0.1ml/kg of 50% Magnesium sulphate – dilute dose 5 times before giving). Can be repeated if necessary.• IV Salbutamol (make up to concentration = 200microgram/ml so 0.3ml/kg/hr=1microgram/kg/min)Loading dose of 15micrograms/kg over 10 minutesMaintenance dose 2-5 micrograms/kg/min
2. Adapted from Scotstar Website M MacKinnon 22.11.2016Raigmore Critical Care GuidelinesPaediatric Asthma GuidelinesFurther Medical Management2nd IV access – regular blood gas, electrolyte and glucose monitoring.• Once on IV salbutamol, nebulised salbutamol should continue every 30 minutes withnebulised ipratropium bromide every 4-6hrs.• IV Aminophylline – if not on long term theophyllines (not to be given via same IV cannula as Salbutamol)Loading dose 5mg/kg over 20 minutesMaintenance dose 1mg/kg/hr Consider IV ondansetron 0.1mg/kg – max dose 4mgCritical Care InterventionEnsure adequate monitoring is in placeIf intubation and ventilation likely, transfer to theatre Consider using ketamine as induction agent (2mg/kg iv, 5-10mg/kg im)Repeat CXR as soon as appropriate following ventilationd/w mike re NIVVentilation StrategiesConsider using SIMV without autoflow as ventilation modeSet extended I:E ratio with relatively low respiratory rateMonitor expiratory flow Monitor intrinsic PEEP to aid setting extrinsic PEEPIf severe air-trapping consider prolonged disconnection from ventilatorConsider ketamine infusion 1-2mg/kg bolus; 0.5-2.5mg/kg/hr (20mg/ml solution saline or dextrose)Consider infusion of muscle relaxant e.g Rocuronium see trolley folderConsider volatile anaesthetic agent (note scavenging issues) Care should be taken to identify signs of salbutamol toxicity particularly in the older age group AcidosisLactataemiaTachycardia/tachyarrhythmias