
A systematic method to determine the pediatric medical actionability for genetic conditions in newborns is needed Many genetic conditions are complex and can complicate the application of any classifying methodology ID: 919501
Download Presentation The PPT/PDF document "Next-generation sequencing for newborn ..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.

Slide1
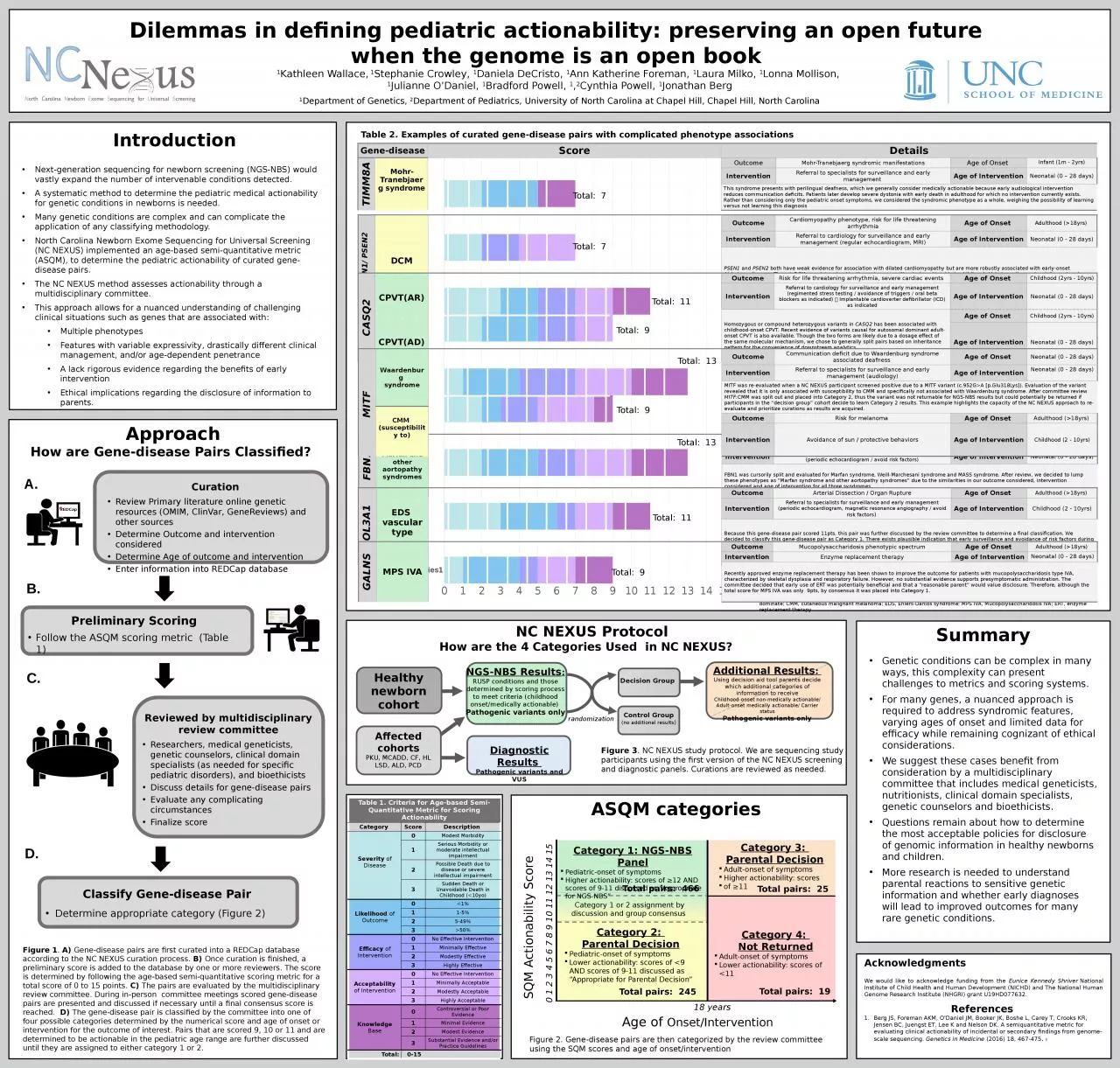
Next-generation sequencing for newborn screening (NGS-NBS) would vastly expand the number of intervenable conditions detected. A systematic method to determine the pediatric medical actionability for genetic conditions in newborns is needed. Many genetic conditions are complex and can complicate the application of any classifying methodology.North Carolina Newborn Exome Sequencing for Universal Screening (NC NEXUS) implemented an age-based semi-quantitative metric (ASQM), to determine the pediatric actionability of curated gene-disease pairs. The NC NEXUS method assesses actionability through a multidisciplinary committee. This approach allows for a nuanced understanding of challenging clinical situations such as genes that are associated with: Multiple phenotypes Features with variable expressivity, drastically different clinical management, and/or age-dependent penetrance A lack rigorous evidence regarding the benefits of early interventionEthical implications regarding the disclosure of information to parents.
Dilemmas in defining pediatric actionability: preserving an open future when the genome is an open book 1Kathleen Wallace, 1Stephanie Crowley, 1Daniela DeCristo, 1Ann Katherine Foreman, 1Laura Milko, 1Lonna Mollison, 1Julianne O’Daniel, 1Bradford Powell, 1,2Cynthia Powell, 1Jonathan Berg1Department of Genetics, 2Department of Pediatrics, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina
Acknowledgments
We
would like to acknowledge funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and The National Human Genome Research Institute (NHGRI) grant U19HD077632.References Berg JS, Foreman AKM, O'Daniel JM, Booker JK, Boshe L, Carey T, Crooks KR, Jensen BC, Juengst ET, Lee K and Nelson DK. A semiquantitative metric for evaluating clinical actionability of incidental or secondary findings from genome- scale sequencing. Genetics in Medicine (2016) 18, 467-475. :
Introduction
SummaryGenetic conditions can be complex in many ways, this complexity can present challenges to metrics and scoring systems. For many genes, a nuanced approach is required to address syndromic features, varying ages of onset and limited data for efficacy while remaining cognizant of ethical considerations. We suggest these cases benefit from consideration by a multidisciplinary committee that includes medical geneticists, nutritionists, clinical domain specialists, genetic counselors and bioethicists. Questions remain about how to determine the most acceptable policies for disclosure of genomic information in healthy newborns and children. More research is needed to understand parental reactions to sensitive genetic information and whether early diagnoses will lead to improved outcomes for many rare genetic conditions.
DCM, dilated cardiomyopathy; CPVT
,
catecholaminergic polymorphic ventricular tachycardia; AR, autosomal recessive; AD, autosomal dominate; CMM, cutaneous malignant melanoma; EDS, Ehlers-Danlos syndrome; MPS IVA, Mucopolysaccharidosis IVA; ERT, enzyme replacement therapy
PSEN1/ PSEN2DCMOutcomeCardiomyopathy phenotype, risk for life threatening arrhythmiaAge of Onset Adulthood (>18yrs) InterventionReferral to cardiology for surveillance and early management (regular echocardiogram, MRI)Age of InterventionNeonatal (0 - 28 days)PSEN1 and PSEN2 both have weak evidence for association with dilated cardiomyopathy but are more robustly associated with early-onset Alzheimer disease. Though DCM was determined by the review committee to be actionable in childhood, Alzheimer disease is adult-onset and considered non-actionable. Ultimately, PSEN1 and PSEN2 were not considered suitable for Category 1 due to a lack of evidence surrounding the variant associated with the DCM phenotype.
CASQ2CPVT(AR)OutcomeRisk for life threatening arrhythmia, severe cardiac events Age of Onset Childhood (2yrs - 10yrs)InterventionReferral to cardiology for surveillance and early management (regimented stress testing / avoidance of triggers / oral beta blockers as indicated) Implantable cardioverter defibrillator (ICD) as indicatedAge of InterventionNeonatal (0 - 28 days)Homozygous or compound heterozygous variants in CASQ2 has been associated with childhood-onset CPVT. Recent evidence of variants causal for autosomal dominant adult-onset CPVT is also available. Though the two forms are likely due to a dosage effect of the same molecular mechanism, we chose to generally split pairs based on inheritance pattern for the convenience of downstream analytics. Age of Onset Childhood (2yrs - 10yrs)CPVT(AD)Age of InterventionNeonatal (0 - 28 days)
FBN1Marfan and other aortopathy syndromesOutcomeRisk for aortic dissectionAge of Onset Variable (no typical range exists)InterventionReferral to cardiology for surveillance and early management (periodic echocardiogram / avoid risk factors)Age of InterventionNeonatal (0 - 28 days)FBN1 was cursorily split and evaluated for Marfan syndrome, Weill-Marchesani syndrome and MASS syndrome. After review, we decided to lump these phenotypes as “Marfan syndrome and other aortopathy syndromes” due to the similarities in our outcome considered, intervention considered and age of intervention for all three syndromes.
COL3A1EDS vascular typeOutcomeArterial Dissection / Organ RuptureAge of Onset Adulthood (>18yrs) InterventionReferral to specialists for surveillance and early management (periodic echocardiogram, magnetic resonance angiography / avoid risk factors) Age of InterventionChildhood (2 - 10yrs)Because this gene-disease pair scored 11pts, this pair was further discussed by the review committee to determine a final classification. We decided to classify this gene-disease pair as Category 1. There exists plausible indication that early surveillance and avoidance of risk factors during pediatric age could confer a net benefit to the patient and family. We recognize the potential of harm this diagnosis carries for an asymptomatic individual and this burden is reflected in a low score for efficacy (1pts) and moderate score for acceptability (2pts) of the intervention.
GALNSMPS IVAOutcomeMucopolysaccharidosis phenotypic spectrumAge of Onset Adulthood (>18yrs) InterventionEnzyme replacement therapyAge of InterventionNeonatal (0 - 28 days)Recently approved enzyme replacement therapy has been shown to improve the outcome for patients with mucopolysaccharidosis type IVA, characterized by skeletal dysplasia and respiratory failure. However, no substantial evidence supports presymptomatic administration. The committee decided that early use of ERT was potentially beneficial and that a “reasonable parent” would value disclosure. Therefore, although the total score for MPS IVA was only 9pts, by consensus it was placed into Category 1.
Table 2. Examples of curated gene-disease pairs with complicated phenotype associations
Gene-diseaseScoreDetailsTIMM8AMohr-Tranebjaerg syndromeOutcomeMohr-Tranebjaerg syndromic manifestationsAge of Onset Infant (1m - 2yrs)InterventionReferral to specialists for surveillance and early management Age of InterventionNeonatal (0 – 28 days)This syndrome presents with perilingual deafness, which we generally consider medically actionable because early audiological intervention reduces communication deficits. Patients later develop severe dystonia with early death in adulthood for which no intervention currently exists. Rather than considering only the pediatric onset symptoms, we considered the syndromic phenotype as a whole, weighing the possibility of learning versus not learning this diagnosis
Total: 7
Total: 7
Total: 11
Total: 9
Total: 13
Total:
9
Total: 13
Total: 11
Total: 9
NC NEXUS Protocol
How
are the 4 Categories Used in NC NEXUS?
Healthy newborn cohort
Diagnostic
Results
Pathogenic variants and VUS
NGS-NBS Results
:
RUSP conditions and those determined by scoring process to meet criteria (childhood onset/medically actionable)
Pathogenic variants only
Control Group
(no additional results
)
Decision
Group
Affected cohorts
PKU, MCADD, CF, HL LSD, ALD, PCD
randomization
Additional Results
:
Using decision aid tool parents decide which additional categories of information to receive
Childhood-onset
non-medically actionable/ Adult-onset medically actionable/ Carrier status
Pathogenic variants only
Figure 3
. NC NEXUS study protocol. We are sequencing study participants using the first version of the NC NEXUS screening and diagnostic panels. Curations are reviewed as needed.
ASQM
categories
SQM Actionability Score
Age of
Onset/Intervention
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
18 years
Category 1: NGS-NBS Panel
Pediatric-onset of symptoms
Higher actionability: scores of ≥12 AND scores of 9-11 discussed as “Appropriate for NGS-NBS”
Category 2:
Parental
Decision
Pediatric-onset of symptoms
Lower actionability: scores of <9 AND scores of 9-11 discussed as “Appropriate for Parental Decision”
Category 3:
Parental Decision
Adult-onset of symptoms
Higher actionability: scores
of ≥11
Category 4:
Not Returned
Adult-onset of symptoms
Lower actionability: scores of <11
Category 1 or 2 assignment by discussion and group consensus
Total pairs: 466
Total pairs: 245
Total pairs: 25
Total pairs: 19
A.
Curation
Review Primary literature online genetic resources (OMIM, ClinVar,
GeneReviews
) and other sources
Determine Outcome and intervention considered
Determine Age of outcome and intervention
Enter information into
REDCap
database
Preliminary Scoring
Follow the ASQM scoring metric (Table 1)
Reviewed by multidisciplinary
review committee
Researchers, medical geneticists, genetic counselors, clinical domain specialists (as needed for specific pediatric disorders), and bioethicists
Discuss details for gene-disease pairs
Evaluate any complicating circumstances
Finalize score
B.
C.
Classify Gene-disease Pair
Determine appropriate category (Figure 2)
D.
Figure 1
.
A)
Gene-disease pairs are first curated into a
REDCap
database according to the NC NEXUS curation process.
B)
Once curation is finished, a preliminary score is added to the database by one or more reviewers. The score is determined by following the age-based semi-quantitative scoring metric for a total score of 0 to 15 points.
C)
The pairs are evaluated by the multidisciplinary review committee. During in-person committee meetings scored gene-disease pairs are presented and discussed if necessary until a final consensus score is reached.
D)
The gene-disease pair is classified by the committee into one of four possible categories determined by the numerical score and age of onset or intervention for the outcome of interest. Pairs that are scored 9, 10 or 11 and are determined to be actionable in the pediatric age range are further discussed until they are assigned to either category 1 or 2.
Approach
How are Gene-disease Pairs Classified?
MITF
Waardenburg
syndrome
Outcome
Communication deficit due to Waardenburg syndrome associated deafness
Age
of Onset
Neonatal (0 - 28 days)
Intervention
Referral to specialists for surveillance and early management (audiology)
Age
of Intervention
Neonatal (0 - 28 days)
MITF was re-evaluated when a NC
NEXUS
participant
screened positive due to a MITF variant (c.952G>A [p.Glu318Lys]). Evaluation of the variant revealed that it is only associated with susceptibility to CMM and specifically not associated with Waardenburg syndrome. After committee review
MITF
:CMM was split out and placed into Category 2, thus the variant was not returnable for NGS-NBS results but could potentially be returned if participants in the “decision group” cohort decide to learn Category 2 results. This example highlights the capacity of the NC NEXUS approach to re-evaluate and prioritize curations as results are acquired.
CMM
(susceptibility to)
Outcome
Risk for melanoma
Age
of Onset
Adulthood (>18yrs)
Intervention
Avoidance of sun / protective behaviors
Age
of Intervention
Childhood (2 - 10yrs)
Table 1. Criteria for Age-based Semi-Quantitative Metric for Scoring Actionability
Category
Score
Description
Severity
of Disease
0
Modest Morbidity
1
Serious Morbidity or moderate intellectual impairment
2
Possible Death due to disease or severe intellectual impairment
3
Sudden Death or Unavoidable Death in Childhood (<10yo)
Likelihood
of Outcome
0
<1%
1
1-5%
2
5-49%
3
>50%
Efficacy
of Intervention
0
No Effective Intervention
1
Minimally Effective
2
Modestly Effective
3
Highly Effective
Acceptability
of Intervention
0
No Effective Intervention
1
Minimally Acceptable
2
Modestly Acceptable
3
Highly Acceptable
Knowledge
Base
0
Controversial or Poor Evidence
1
Minimal Evidence
2
Modest Evidence
3
Substantial Evidence and/or Practice Guidelines
Total:
0-15
Figure 2. Gene-disease
pairs are then categorized by the review committee using the SQM scores and age of onset/intervention