
Gestational or pregnancyassociated breast cancer is defined as breast cancer that is diagnosed during pregnancy in the first postpartum year or any time during lactation Up to 20 percent of breast cancers in women under age 30 are pregnancy associated ID: 915741
Download Presentation The PPT/PDF document "Gestational or pregnancy-associated brea..." is the property of its rightful owner. Permission is granted to download and print the materials on this web site for personal, non-commercial use only, and to display it on your personal computer provided you do not modify the materials and that you retain all copyright notices contained in the materials. By downloading content from our website, you accept the terms of this agreement.




Slide1
Gestational or pregnancy-associated breast cancer
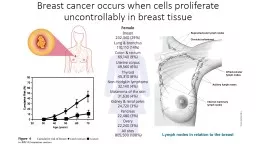
Slide2Gestational or pregnancy-associated breast cancer
is defined as breast cancer that is diagnosed during pregnancy, in the first postpartum year, or any time during lactation.
Up to 20 percent of breast cancers in women under age 30 are pregnancy associated
Slide3The patient was a
32
year
old
female
past
medical history who presented to breast
clinic due to breast lump.
At time of presentation patient was in the 3rd trimester of her 4th pregnancy (G4P3). She first noticed the palpable mass 1 month prior.
Patient
had ultrasound evaluation of both breasts prior to clinic visit in
which
showed 2.8 x 1.8 x 2.7 cm irregular mass at the 8 o’ clock position 7 to 8 cm from the nipple of the right breast
Slide4Slide5Exam was positive for a palpable mass in the right breast located in the lower outer quadrant measuring 2.5 cm.
The
mass was mobile and well circumscribed. No skin changes or nipple discharge were noted.
The
right
axilla
was without
lymphadenopathy
.
Exam was also positive for a gravid abdomen consistent with gestational age for her 3rd trimester
Slide6Primary tumor
The
physiologic changes in the breast
that accompany pregnancy (
eg
, engorgement and hypertrophy) make
physical examination
more challenging, interpretation of findings more difficult, and may limit the utility of mammography
Slide7Mammography
Mammography is
not contraindicated
in pregnancy as the average glandular dose to the breast for a two-view mammogram (200 to 400
millirad
) provides a negligible radiation dose to the fetus as long as abdominal
shielding
is used
Slide8Ultrasonography
Breast
ultrasonography
can determine whether a breast mass is a simple or complex
cyst or a solid
tumor without the risk of fetal radiation exposure and may be used to guide the diagnostic biopsy.
A
focal solid mass
is observed in the majority of cases of gestational breast cancer
Slide9Breast MRI
Gadolinium-enhanced MRI
appears to be more
sensitive
than mammography for detecting invasive breast cancer, particularly in women with dense breast tissue.
Studies demonstrate potential fetal harm with gadolinium exposure in the first trimester
Gadolinium
should therefore be
avoided
during pregnancy if possible
Slide10Biopsy
A clinically suspicious breast mass requires biopsy for definitive diagnosis
, regardless of whether or not a woman is pregnant and despite negative mammographic or ultrasound findings.
Core,
incisional
, or
excisional
biopsies can be performed relatively safely during pregnancy, preferably under local anesthesia
Needle core biopsy
is the preferred method.
Slide11No masses were seen in the left breast. She then underwent ultrasound guided core biopsy of the right breast.
Pathology
showed
invasive
ductal
carcinoma (Grade III, moderate to poorly differentiated) with a malignant
stromal
component consistent with
metaplastic
carcinoma
(
carcinosarcoma
).
Receptors
were ER, PR and Her2 negative.
Slide12PATHOLOGIC FEATURES
The majority of breast cancers in pregnant women are
infiltrating
ductal
adenocarcinomas
as in
nonpregnant
women.
However, pregnancy-associated breast cancers are predominantly
poorly differentiated
and diagnosed at an
advanced stage
, particularly in those diagnosed while lactating
Slide13Hormone receptor expression
Most series report a
lower frequency of estrogen receptor and progesterone receptor
expression in pregnancy-associated breast cancer compared with breast cancer in
nonpregnant
patients (approximately 25 versus 55 to 60 percent)
Slide14It was decided that the patient should undergo
neoadjuvant
chemotherapy
as soon as possible as she was in the 3rd trimester.
Slide15Staging
Chest computed tomography
(CT) scans are generally avoided during pregnancy
If further evaluation of the chest is warranted, an MRI of the thorax is preferred.
Abdominal ultrasound
for the evaluation of liver metastases is a safe procedure in pregnant women but is significantly less sensitive than CT or MRI
MRI without contrast
is preferred if further visceral organ evaluation is required
Bone evaluation
— Radionuclide bone scans are reported to be safe during pregnancy
Slide16MONITORING OF THE PREGNANCY
The pregnant woman with breast cancer requires careful and continuous monitoring of her pregnancy by her obstetrician (often a specialist in maternal and fetal medicine) and her oncologist.
Confirmation of gestational age and expected date of delivery are important as both are significant factors in treatment planning.
Amniocentesis may be required to determine pulmonary maturity if early delivery is being considered
Slide17Slide18Systemic therapy
The data suggest it is safe to administer many agents used in the treatment of breast cancer during pregnancy when initiated
after the first trimester
, and that the majority of pregnancies result in live births with low related morbidity in the newborns
The most data available are with
anthracycline
-based chemotherapy
, often on an every-three-week schedule.
Taxanes
appears feasible and safe during the second and third trimesters of pregnancy, with minimal maternal, fetal, or neonatal toxicity
The use of
trastuzumab
during pregnancy is
contraindicated.
The use of selective estrogen receptor modulators (SERMs) such as
tamoxifen
during pregnancy is generally
avoided
Slide19Timing of chemotherapy
For pregnant breast cancer patients who need chemotherapy treatment, clinicians should
advise against a delay
in the initiation of systemic chemotherapy once the pregnancy has safely reached the
second or third trimester
Care needs to be taken to avoid exposing the fetus to chemotherapy during the first trimester, and to stop chemotherapy prior to delivery so that the mother and infant are not experiencing treatment-related toxicities in the delivery or postpartum stages
Slide20She then received 4 cycles of
Adriamycin
and
Cytoxan
.
Roughly at the end of the
chemotherapy treatment the patient had a repeat breast ultrasound which showed the mass to be increased in size to 5.1 x 3.7 x 5.1 cm
Slide21Locoregional treatment
The same local treatment options that are available for
nonpregnant
patients should be considered in pregnant women, with the
exception of radiation therapy (RT)
Slide22Mastectomy
Mastectomy may be chosen when the patient opts to continue the pregnancy, even for women with clinical anatomic stage I and II disease
An advantage of mastectomy may be the
elimination of the need for breast RT
Slide23Breast-conserving surgery
The therapeutic equivalence of mastectomy and breast-conserving therapy (breast-conserving surgery [BCS] followed by RT) has been demonstrated in
nonpregnant
women; this is also true for the pregnant patient.
BCS can be used effectively as
RT
can be
delayed
after the administration of adjuvant or
neoadjuvant
chemotherapy.
Slide24Radiation therapy
Radiation should be
delayed
whenever possible until
after delivery.
Slide25Management of the axilla
The use of
sentinel lymph node biopsies
during pregnancy is controversial, with case series demonstrating increasing evidence of safety and efficacy in pregnant patients
Therefore,
axillary
lymph node dissection
should be considered as
standard
approach.
Slide26she
was taken for a right skin sparing mastectomy with right
axillary
sentinel lymph node biopsy
and
placement of tissue expander.
Of
the 3 sentinel lymph nodes taken all were negative
.
Final pathology of the mass showed
metaplastic
carcinoma (
carcinosarcoma
).
The
epithelial component was invasive
ductal
carcinoma grade III/III (Mitotic rate 3, Nuclear
pleomorphism
3, Glandular/Tubular differentiation 2,
Histologic
grade 3) and the
mesenchymal
component was poorly differentiated sarcoma.
The
mass was 6.2 cm at the widest diameter with necrosis and areas of infarct present. Final tumor stage was pT3N0Mx, Stage IIB, ER (+) (<5%), PR (-), Her2 (-).
Patient
had genetic testing and was found to be BRCA (-).
Slide27Timing of delivery
Delivery should occur
following
the mother's white blood cell count and platelet count
nadir
to reduce the potential risk of infectious complications and bleeding from thrombocytopenia.
Chemotherapy should be
avoided for three to four weeks
before delivery to avoid transient neonatal
myelosuppression
and potential complications of sepsis and death whenever possible.
Slide28Elective termination of pregnancy
The decision to continue or terminate the pregnancy should be individualized and made by a fully informed woman in conjunction with her clinician.
Early termination of pregnancy does not improve the outcome of gestational breast cancer
Slide29Maternal health
Contemporary studies that specifically evaluated the outcomes of women diagnosed with breast cancer
during
pregnancy have consistently shown that there is
no negative impact
on survival
Slide30PREGNANCY AFTER BREAST CANCER
Pregnancy in breast cancer survivors did not significantly impact survival and suggested that pregnancy after breast cancer may have a
protective effect
It is common for clinicians to advise women to wait for at least
two years
before contemplating pregnancy
The primary reason for this recommendation is that most
recurrences
of breast cancer occur within the
first two years
after initial diagnosis and treatment
Slide31Thanks for your patient attention